Recognizing is crucial for understanding the severe manifestations of spinal curvature. Visual identification of these advanced signs can aid in early referral and appropriate management planning for individuals experiencing significant spinal deformity.
grade 3 scoliosis Symptoms Pictures
The visual presentation of typically reveals profound and unmistakable changes to the body’s symmetry and posture. At this advanced stage, characterized by a Cobb angle often exceeding 45-50 degrees, the structural alterations to the spine are clearly evident, impacting the torso, shoulders, and hips. These visible cues are critical for clinical assessment and for individuals to recognize the severity of their condition. The deformation is not merely aesthetic; it signifies significant structural changes that can impinge on organ function and overall quality of life. Understanding these is the first step toward effective intervention.
Key observable in grade 3 scoliosis include:
- : One shoulder appears significantly higher than the other. This asymmetry is often one of the most striking , particularly when viewed from the front or back. The elevation can be substantial, pulling the neck and collarbone into an altered position.
- : When bending forward (Adam’s Forward Bend Test), a notable hump becomes visible on one side of the back, primarily due to the rotation of the spine causing the ribs to protrude. This is a hallmark of rotational deformity and is crucial for identifying structural scoliosis. Even without bending, a subtle or obvious rib cage asymmetry can be observed, where one side of the back or chest appears fuller or higher.
- : One side of the waist may appear to have a sharper curve or be more indented than the other, creating a noticeable asymmetry. Concurrently, one hip often appears higher or more prominent, throwing the pelvis out of alignment. This impacts gait and balance.
- : In severe cases, the head may visibly lean to one side or appear off-center when aligned with the pelvis, indicating significant compensatory curves in the neck and upper back. This head tilt is a direct consequence of the body attempting to maintain balance despite the spinal curvature.
- : The actual curve of the spine can often be seen or palpated through the skin, presenting as an ‘S’ or ‘C’ shape along the back. This can be quite pronounced, especially in individuals with thinner body types. The severity of the curvature is what defines grade 3 scoliosis.
- : The entire torso may appear shifted laterally to one side relative to the pelvis, further emphasizing the body’s attempt to compensate for the severe spinal curve and maintain equilibrium. This is a clear indicator of structural imbalance.
- : Garments, especially shirts and jackets, may hang unevenly, with one sleeve appearing longer or one side of the collar sitting higher. Pants may also appear to have one leg longer than the other, or one side of the waistband may sit higher on the hip. This is a practical and everyday sign of .
- : Due to the rotational and lateral forces on the spine, muscles on one side of the back may appear more developed or taut, while muscles on the other side may appear stretched or atrophied. This muscular imbalance contributes to pain and further postural deviation.
- : In some cases, especially if the curve affects the thoracic spine significantly, one shoulder blade (scapula) may protrude more prominently from the back, often referred to as a “winged scapula.” This is due to changes in rib cage mechanics and muscle attachments.
- : The severe spinal deformity can lead to an altered gait, with individuals potentially shifting their weight unevenly or struggling with balance. This can manifest as a subtle limp or an awkward walking pattern, reflecting the body’s struggle to maintain stability with a severely distorted axis.
These offer a comprehensive view of the visual indicators of severe scoliosis. Early and accurate identification of these signs is vital for guiding treatment decisions and improving patient outcomes, highlighting the importance of regular spinal screenings, especially during adolescent growth spurts.
Signs of grade 3 scoliosis Pictures
Beyond the general symptoms, specific provide objective evidence of the spinal deformity’s advanced state. These signs are typically observed during a physical examination and are critical for a definitive diagnosis and treatment planning. The objective assessment of these helps differentiate grade 3 scoliosis from milder forms and other musculoskeletal conditions. Clinicians look for a constellation of findings that collectively point to a significant structural alteration of the vertebral column, often accompanied by vertebral rotation and rib cage distortion.
Detailed include:
- :
- : When the patient bends forward at the waist, with arms hanging loosely and knees straight, a distinct, often large, prominence on one side of the back (a rib hump) is a definitive sign. This is caused by the rotation of the vertebrae, which pulls the attached ribs posteriorly on the convex side of the curve. This is usually the most striking visual sign during this test.
- : One side of the waist may show a deeper crease or indentation than the other due to the lateral deviation of the spine and the associated soft tissue changes.
- : One scapula (shoulder blade) may be noticeably higher or protrude more than the other, further highlighting the thoracic asymmetry.
- :
- : A significant difference in the height of the shoulders, often with one shoulder appearing much higher and sometimes protracted. This is a common and easily observable sign.
- : The curve of the waist on one side is starkly different from the other, often creating a deep C-shape on one side and a flattened appearance on the other. This indicates substantial trunk deviation.
- : While not a true leg length difference, the pelvic tilt caused by the scoliosis can make one leg appear shorter than the other, leading to compensatory changes in gait.
- : The entire upper body is visibly shifted to one side relative to the midline of the pelvis, indicative of a large decompensated curve. This is a critical indicator of severe imbalance.
- : One hip bone (iliac crest) may be significantly higher or more outward-flaring compared to the other, making pants or skirts fit unevenly.
- :
- During palpation, the spinous processes of the vertebrae may be felt deviating significantly from the midline.
- Muscle tightness and prominence may be noted on the convex side of the curve, while the concave side might feel stretched or atrophied. This muscular imbalance is often a source of .
- :
- : Numbness, tingling, or altered sensation in the extremities can occur if the severe curvature compresses spinal nerves.
- : Weakness in specific muscle groups supplied by compressed nerves is a serious sign, indicating potential neurological compromise.
- : Diminished or exaggerated deep tendon reflexes can also point to neurological involvement, requiring urgent assessment.
- :
- : Significant thoracic curves (often >70-80 degrees, but can begin impacting in grade 3 range) can restrict lung capacity, leading to breathlessness, especially with exertion. This is a severe .
- : Non-cardiac chest pain can arise from the mechanical stress on the rib cage and intercostal muscles due to severe deformity.
- : Reduced cardiorespiratory efficiency can lead to chronic fatigue.
These detailed highlight the profound impact of severe scoliosis on the musculoskeletal and potentially cardiorespiratory systems. Thorough clinical evaluation is essential to identify these signs and implement an appropriate management strategy, which frequently involves surgical intervention for curves of this magnitude.
Early grade 3 scoliosis Photos
While “grade 3 scoliosis” by definition refers to a severe curvature (typically >45-50 degrees Cobb angle), the concept of “” must be understood as the visual cues indicating the *progression* towards this severe stage, or the identification of initial, milder curves that are at high risk of progressing rapidly to grade 3. It’s about recognizing the before it becomes a full-blown severe deformity. Early detection and intervention are paramount to potentially alter the natural history of the curve, minimizing the chances of it reaching grade 3 or reducing its severity if it does.
Identifying these in pre-adolescents and adolescents is crucial:
- :
- Initially, the difference in shoulder height might be minimal, perhaps only an inch or two, and easily overlooked. One shoulder may just appear slightly higher or more rounded than the other. This often becomes more apparent when the individual is shirtless.
- Parents might notice that shirt necklines seem to pull to one side or that one sleeve appears longer.
- :
- In the early stages, the rib hump might be very subtle, a slight elevation rather than a pronounced protrusion. This requires a keen eye during spinal screenings.
- The test should be performed with careful observation from both the front and back to catch these minimal asymmetries.
- :
- A minor difference in the contour of the waist on either side, perhaps one side appearing a little flatter or with a slightly sharper curve, can be an early indicator. This might be missed if not specifically looked for.
- The “C” or “S” shape is not yet stark, but the beginning of deviation is present.
- :
- The body might show a tendency to lean slightly to one side, or the head may not be perfectly centered over the pelvis when standing upright. This can be an initial sign of a developing compensatory curve.
- Often, the individual might unconsciously adjust their posture to compensate, making it harder to spot.
- :
- While not as dramatic as in grade 3, clothing might start to fit a little unevenly. One pant leg might seem to drag, or a shirt hem might appear slightly askew. This is often one of the first things family members or friends notice.
- Bras might not sit evenly, or backpack straps might consistently slide off one shoulder.
- :
- While scoliosis is often painless in early stages, some individuals may experience intermittent, mild back discomfort or fatigue in the spinal region, particularly after prolonged standing or physical activity. This can sometimes be attributed to muscle strain attempting to stabilize the spine.
- It’s important to distinguish this from general growing pains.
- :
- A slight prominence or “winging” of one shoulder blade, where the inner border lifts away from the chest wall, can sometimes be an early sign, especially with thoracic curves.
The significance of recognizing these cannot be overstated. For a curve that is already showing progression, even if still mild to moderate (e.g., 20-40 degrees), its trajectory toward grade 3 (requiring surgical consideration) can be predicted by factors such as patient age, gender, skeletal maturity, and curve pattern. Early intervention, such as bracing, if appropriate for curves between 20-40 degrees in growing adolescents, aims to halt or slow this progression, thereby preventing the severe deformities associated with grade 3 scoliosis. Regular monitoring by a specialist with follow-up X-rays is critical for any curve deemed at risk of progression.
Skin rash grade 3 scoliosis Images
It is important to clarify that itself, being a structural deformity of the spine, does not directly cause skin rashes. However, certain underlying genetic syndromes or conditions that are associated with a higher incidence of scoliosis can manifest with distinct . When discussing , we are typically referring to these associated systemic conditions whose cutaneous manifestations might be observed concurrently with a severe spinal curvature. Recognizing these specific skin signs is vital, as they can provide clues to the etiology of the scoliosis, influencing diagnosis, prognosis, and management strategies. The presence of these skin findings can indicate a syndromic form of scoliosis, which may have different progression patterns or associated systemic issues.
The most prominent associated condition with both scoliosis and characteristic skin findings is . Other conditions, though less common or with less pronounced skin signs directly linked to “rash,” include Marfan syndrome (striae) and Ehlers-Danlos syndrome (hyperextensible skin, poor wound healing).
Key (especially NF1) that clinicians look for include:
- :
- : These are flat, uniformly hyperpigmented (light brown to dark brown) spots on the skin. They are typically oval or irregular in shape with smooth borders. The color is often compared to “coffee with milk.”
- : While a single CALM is common, the presence of with a diameter of 5 mm or larger in prepubertal individuals, or 15 mm or larger in postpubertal individuals, is a major diagnostic criterion for NF1.
- : They can appear anywhere on the body, but are often prominent on the trunk and extremities.
- : NF1 is one of the most common causes of syndromic scoliosis, with a significant percentage of NF1 patients developing spinal deformities, sometimes severe enough to reach grade 3. The presence of CALMs alongside scoliosis should strongly prompt investigation for NF1.
- :
- : These are clusters of small, freckle-like spots that appear in the armpit (axillary) or groin (inguinal) regions. They are distinct from typical sun-induced freckles.
- : Crowe’s sign is highly specific for NF1. The appearance of these freckles is often diagnostic, even in the absence of numerous CALMs.
- : Confined to skin folds, particularly the axilla and groin.
- : Similar to CALMs, these freckles are a strong indicator of NF1 and thus suggest that any accompanying scoliosis may be neurofibromatosis-associated scoliosis, which often has unique characteristics (e.g., dystrophic vs. non-dystrophic) and can be more aggressive.
- :
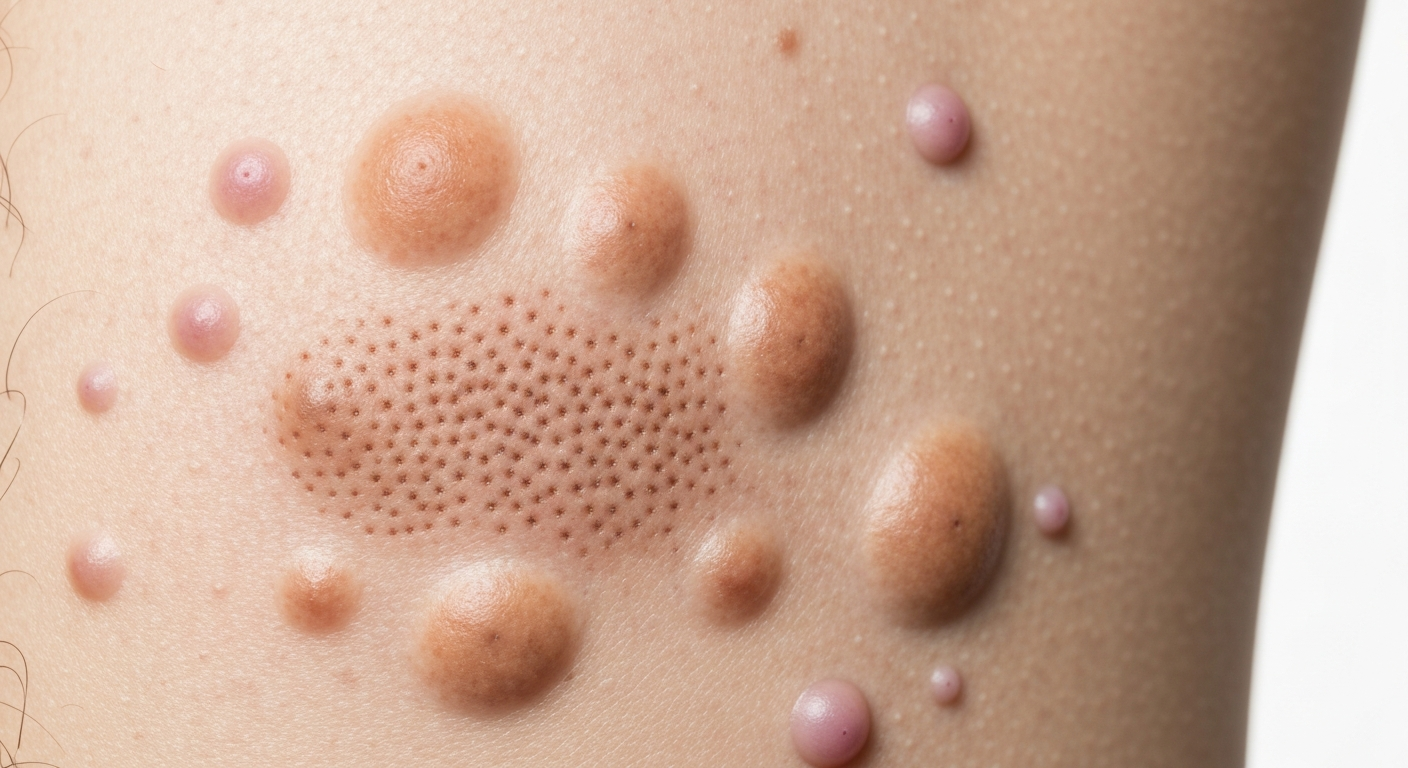
- : These are benign, soft, flesh-colored to purplish, dome-shaped or pedunculated (stalked) tumors that grow on or under the skin. They can vary widely in size and number, from a few to hundreds. They often feel soft and rubbery.
- : Multiple cutaneous neurofibromas are a diagnostic criterion for NF1. They typically appear later in childhood or adolescence.
- : Can be found anywhere on the body.
- : Their presence further solidifies an NF1 diagnosis in a patient with scoliosis, guiding management towards potential neurological or other systemic complications of NF1.
- :
- : These are larger, often deeper, more diffuse neurofibromas that can involve multiple nerve bundles and surrounding tissues. They can cause significant disfigurement and nerve compression. They often feel like a “bag of worms” on palpation.
- : While not a “rash,” these are significant skin/subcutaneous findings in NF1.
- : Can occur anywhere, including along nerve roots close to the spine.
- : Plexiform neurofibromas located near the spine can directly contribute to or exacerbate scoliosis development, especially if they cause vertebral erosion or dural ectasia, making the scoliosis more complex and challenging to treat.
- :
- : These are purplish-red linear skin lesions that evolve into silvery-white stretch marks, often appearing without a history of significant weight change or pregnancy.
- : While not a primary diagnostic criterion, are a minor criterion for Marfan syndrome, a connective tissue disorder.
- : Commonly found over the shoulders, hips, and lower back.
- : Marfan syndrome is frequently associated with scoliosis, often rapidly progressive and severe (grade 3), due to generalized connective tissue laxity. The presence of striae alongside severe scoliosis can suggest Marfan’s and prompt further cardiovascular and ocular evaluation.
In summary, while there isn’t a “grade 3 scoliosis rash” per se, the presence of specific in a patient with severe scoliosis points towards an underlying syndromic cause. These visual clues are critical for comprehensive diagnosis and patient care, allowing for targeted screening for other systemic manifestations and often influencing the surgical approach and long-term prognosis of the scoliosis.
grade 3 scoliosis Treatment
is typically multidisciplinary and almost always involves surgical intervention due to the severity of the spinal curve, which generally exceeds 45-50 degrees Cobb angle in skeletally immature individuals or 50 degrees in mature individuals. At this stage, the risk of further progression is very high, and the deformity can impact vital organ function (e.g., cardiopulmonary compromise in severe thoracic curves) and quality of life. The primary goal of is to correct the spinal deformity as much as safely possible, prevent further progression, alleviate pain, improve balance and posture, and protect neurological and cardiopulmonary function.
The comprehensive approach to includes:
- :
- : Spinal fusion is the gold standard for . It involves surgically joining (fusing) two or more vertebrae together so that they heal into a single, solid bone. This eliminates motion between the fused vertebrae, thereby preventing further curve progression. Metal rods, screws, and hooks are typically used to hold the spine in a straighter position during the fusion process. Bone graft material (autograft from the patient or allograft from a donor) is used to facilitate the fusion.
- :
- : This is the most common approach, performed from the back. It allows for excellent visualization of the spine and effective correction. Instrumentation is placed along the posterior elements of the vertebrae.
- : Less common for primary scoliosis in grade 3 but sometimes used for specific thoracolumbar curves or in conjunction with posterior fusion. It involves accessing the spine from the front (chest or abdomen). This approach can be beneficial for certain curve types as it can achieve excellent correction and potentially fewer fused levels.
- : In extremely severe or rigid curves, or for certain types of kyphoscoliosis, both anterior and posterior approaches may be used in a single or staged procedure to achieve maximum correction and stability.
- : While historically used for more flexible curves in growing patients, some advancements are exploring its role in highly selected, more advanced cases. It’s a growth modulation technique where a strong, flexible cord is implanted along the convex side of the curve, allowing continued growth on the concave side to correct the curve. It’s considered a “fusionless” option, but its application for established grade 3 curves is limited and still evolving.
- :
- : Reduce the Cobb angle significantly, typically aiming for 50-70% correction or more.
- : Halt further worsening of the curve.
- : Improve the alignment of the head, trunk, and pelvis.
- : Reduce the appearance of the rib hump and other deformities, leading to better body image.
- : Address pain directly caused by the spinal deformity or muscle imbalance.
- : Prevent or relieve pressure on the spinal cord or nerve roots.
- : In severe thoracic curves, surgery can expand lung capacity and improve breathing.
- :
- Infection
- Bleeding (requiring blood transfusion)
- Neurological injury (spinal cord or nerve damage, though rare with modern monitoring)
- Pseudarthrosis (failure of the vertebrae to fuse)
- Hardware malfunction (e.g., rod breakage, screw pullout)
- Pain at the bone graft site
- Adjacent segment disease (degeneration of unfused segments above or below the fusion)
- Pulmonary complications
- Implant prominence or irritation
- :
- : Including cardiac and pulmonary assessments, especially important if there are concerns about organ function due to the severe curve.
- : To establish baseline function.
- : To aid in healing.
- : To prepare the patient and family for surgery and recovery.
- : To optimize strength and flexibility.
- :
- : Crucial in the immediate post-operative period.
- : Encouraging walking soon after surgery to prevent complications and promote recovery.
- : Guided exercises to restore strength, flexibility, and improve posture. PT is essential for long-term recovery and adaptation to the new spinal alignment.
- : Avoiding heavy lifting, bending, and twisting for several months to allow solid fusion to occur.
- : With X-rays to monitor fusion progress and overall recovery.
- :
- : For chronic pain that may persist or arise from muscular imbalances, physical therapy, exercise, medication (NSAIDs, muscle relaxants), and alternative therapies (acupuncture, massage) can be used. These are typically used as adjuncts to manage symptoms, not to correct the curve itself.
- : While not correcting the curve, targeted exercises can strengthen core muscles, improve flexibility, and enhance overall functional capacity. This is often an integral part of pre- and post-operative care and can help manage symptoms in the long term.
- : Bracing is primarily effective for preventing progression in moderate curves (25-45 degrees) in growing adolescents. Once a curve reaches magnitude, bracing is usually ineffective at achieving significant correction or halting progression. It might occasionally be used post-surgery in some protocols, or for symptom management in very specific adult cases where surgery is contraindicated, but it is not a primary treatment for severe pediatric scoliosis curves.
The decision for is highly individualized, considering the patient’s age, skeletal maturity, curve magnitude and pattern, progression rate, presence of pain, and impact on daily life and organ function. A comprehensive evaluation by an experienced spinal surgeon and a multidisciplinary team is essential to determine the most appropriate for optimal outcomes.