Understanding Stomach ulcer symptoms pictures is crucial for early detection and effective management. This article provides detailed descriptions of various manifestations of stomach ulcers, focusing on what patients and clinicians might observe or experience. We delve into the visual cues and symptomatic indicators that signal the presence of this common gastrointestinal condition, offering comprehensive insights into its progression and associated signs.
Stomach ulcer Symptoms Pictures
When considering Stomach ulcer symptoms pictures, it’s important to visualize the internal and external manifestations. The most prominent symptom is a burning, gnawing pain in the upper abdomen, often described as a hunger pain. This epigastric pain typically occurs between meals or during the night, subsiding temporarily after eating or taking antacids. A visual representation of a patient experiencing this pain might show them clutching their upper abdomen, indicating the discomfort. The pain can be sharp, dull, or aching, and it often radiates to the back or chest, giving a sensation of chest discomfort or back pain associated with peptic ulcer disease. The timing of the pain is a key diagnostic indicator for gastric ulcers; it often worsens immediately after eating, especially with acidic or spicy foods, unlike duodenal ulcers which may be relieved by food. This post-meal exacerbation can lead to a fear of eating, resulting in unintentional weight loss, a visible sign of chronic illness.
Other significant symptoms that might be inferred from Stomach ulcer symptoms pictures include nausea and vomiting. Nausea is a common complaint, often persistent and accompanied by a feeling of fullness. Vomiting can provide temporary relief from pain and is more common with gastric outlet obstruction, a severe complication where the ulcer blocks the passage of food from the stomach. If vomiting occurs, the vomitus might contain blood, appearing as bright red hematemesis or dark “coffee ground” material, indicating upper gastrointestinal bleeding. This is a critical sign requiring immediate medical attention, and images depicting such vomitus would highlight the severity of the ulcer complication. Similarly, changes in bowel habits can be telling. Melena, dark, tarry stools, is a visual indicator of digested blood from an upper GI bleed, while hematochezia (bright red blood in stool) is less common but can occur with very rapid or large bleeds. These visible stool changes are strong indicators of bleeding ulcer complications and necessitate urgent medical evaluation for peptic ulcer diagnosis.
Beyond pain, dyspepsia symptoms are frequently reported. These include bloating, abdominal distension, early satiety (feeling full after eating only a small amount of food), and excessive belching or burping. While not directly visible on a standard photograph, a patient’s posture or facial expression could convey these discomforts. For instance, a person constantly rubbing their stomach or appearing visibly uncomfortable after a meal might suggest these ulcer symptoms. Loss of appetite (anorexia) is another common symptom, driven by both the discomfort of eating and the underlying disease process. Chronic fatigue and weakness can also be present due to continuous pain, poor nutrient absorption, or blood loss, manifesting as a general pallor or lack of energy visible in a patient’s appearance. These various manifestations underscore the complex nature of stomach ulcer presentation and the importance of recognizing the full spectrum of signs for effective ulcer treatment.
Signs of Stomach ulcer Pictures
Delving into Signs of Stomach ulcer Pictures often involves understanding both overt physical indicators and the internal visual evidence provided by medical imaging. From a clinical perspective, certain signs alert healthcare providers to the presence of peptic ulcer disease or its complications. For instance, pallor or pale skin, lips, and conjunctivae can be a significant sign of anemia resulting from chronic, slow blood loss from an ulcer. A picture highlighting the pale complexion of an individual suffering from prolonged gastrointestinal bleeding would strongly suggest this complication. This anemic appearance is a critical visual cue for ulcer evaluation.
In cases of severe bleeding, more dramatic signs might be evident. Hematemesis, the vomiting of blood, can be explicitly captured. Pictures showing bright red blood or dark, granular “coffee grounds” in vomitus are unmistakable signs of active upper GI bleeding, often originating from a bleeding gastric ulcer. Similarly, melena, characterized by sticky, tarry-black stools, is a visual sign of digested blood and indicates a significant bleed higher in the gastrointestinal tract. A detailed image of melenic stool provides crucial diagnostic information for ulcer complications. Other systemic signs related to significant blood loss include tachycardia (rapid heart rate), hypotension (low blood pressure), and signs of hypovolemic shock such as cool, clammy skin and altered mental status – visual representations of these would emphasize the severity of the bleeding crisis associated with perforated ulcer or a deeply eroding ulcer.
For individuals with gastric outlet obstruction due to an ulcer, abdominal distension and visible peristaltic waves across the abdomen might be observed. These waves represent the stomach trying to push food through a narrowed pylorus and are a direct visual sign of obstruction. Succession splash, a sloshing sound heard over the stomach on auscultation, is another sign, though not directly pictured. If an ulcer perforates, leading to peritonitis, the abdomen becomes exquisitely tender, rigid, and “board-like.” A patient in this state would likely be curled up, guarding their abdomen, exhibiting severe distress and immobility. This acute abdomen presentation is a medical emergency requiring immediate surgical intervention. Radiographic images, such as an upright chest X-ray, showing free air under the diaphragm (pneumoperitoneum) are definitive visual proof of a perforated ulcer.
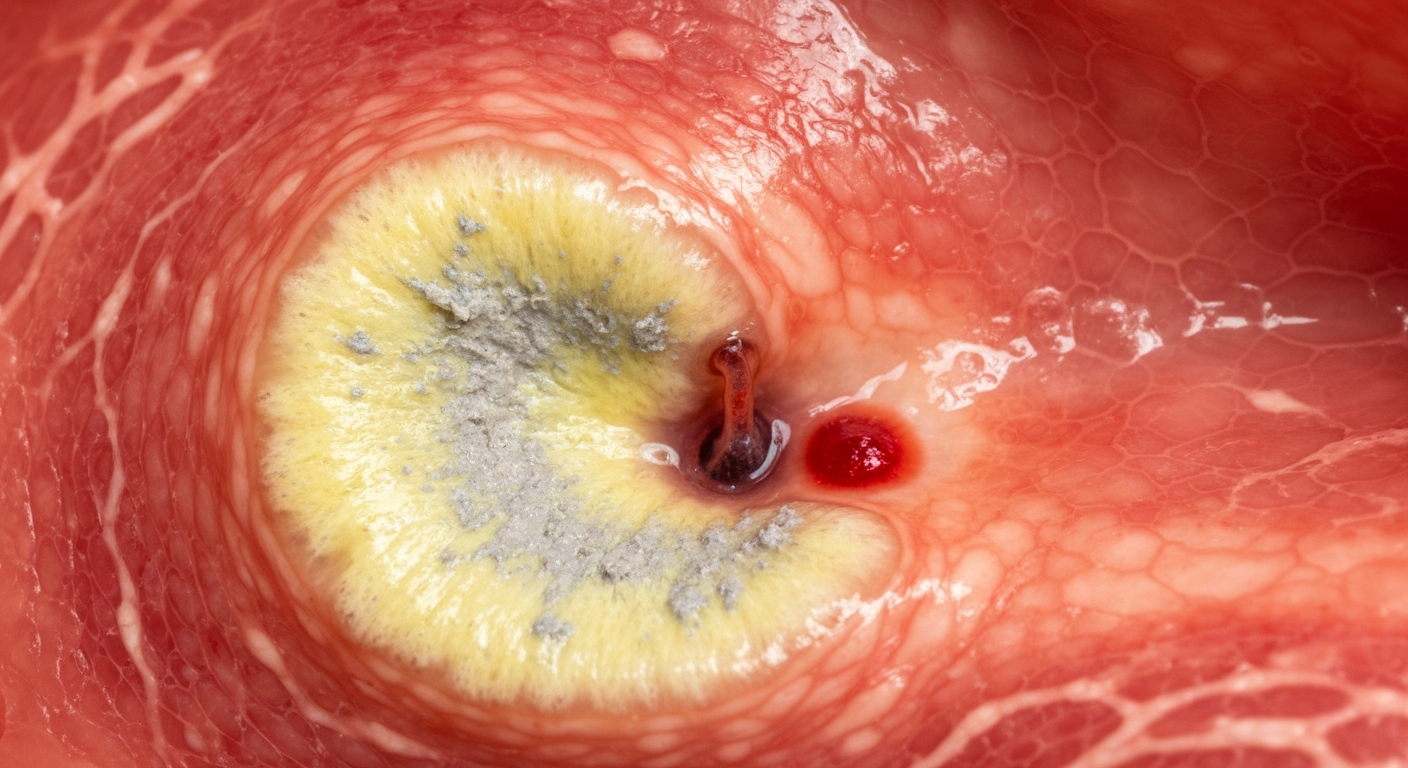
Endoscopy provides the most direct visual diagnosis of ulcers. Endoscopic images of stomach ulcers reveal distinct characteristics:
Ulcer Crater: A well-demarcated depression or hole in the gastric mucosa. The size can vary from a few millimeters to several centimeters.
Ulcer Base: Often covered with a white or yellow exudate (fibrin, necrotic tissue), which can appear greyish or sloughing.
Surrounding Mucosa: Typically inflamed, erythematous (reddened), and edematous (swollen).
Bleeding Stigmata: In cases of bleeding ulcers, endoscopic images might show:
Active arterial spurting: A visible jet of blood from a vessel in the ulcer base.
Non-bleeding visible vessel: A dark spot or protuberance in the ulcer base, indicating an exposed vessel with a high risk of re-bleeding.
Adherent clot: A clot firmly attached to the ulcer base, also a sign of recent bleeding.
Flat spot: A dark red or black spot, indicating recent hemorrhage.
Edge Characteristics: The edges of a benign ulcer are usually smooth and regular, whereas irregular, raised, or nodular edges can suggest malignancy, necessitating biopsies for ulcer differentiation.
These endoscopic findings are crucial for stomach ulcer diagnosis and guiding appropriate ulcer treatment strategies.
Early Stomach ulcer Photos
Understanding Early Stomach ulcer Photos requires a focus on the initial, less severe manifestations of the condition, often detectable during an upper endoscopy. While patients may experience subtle symptoms, the visual evidence under endoscopy provides concrete proof of developing mucosal injury. In the earliest stages, a stomach ulcer may not appear as a deep crater but rather as more superficial lesions or areas of significant inflammation. These early gastric lesions are vital for prompt early ulcer diagnosis and intervention to prevent progression to more severe stages.
Common early visual signs of an ulcer during endoscopy include:
Erosions: These are superficial breaks in the gastric mucosa that do not penetrate the muscularis mucosae layer. They appear as small, often multiple, reddish areas with a whitish base, sometimes slightly depressed. While not full ulcers, extensive erosions indicate significant mucosal damage and can precede ulcer formation, especially in cases of NSAID-induced gastropathy or severe stress. An image depicting scattered reddish patches on the stomach lining would represent these erosions, signifying early gastric mucosal injury.
Shallow Ulcerations: These are slightly deeper than erosions, penetrating the muscularis mucosae but often still relatively small (e.g., <5 mm) and less defined than chronic ulcers. They may have a thin layer of exudate or fibrin, and the surrounding mucosa might appear only mildly inflamed. Pictures of such shallow defects offer valuable insight into the initial ulcer development.
The surrounding gastric mucosa in early ulcers often shows signs of inflammation (gastritis). This can manifest as:
Erythema: Reddening of the stomach lining, indicating increased blood flow due to inflammation.
Edema: Swelling of the mucosal folds, making them appear thicker and blunted.
Friability: The mucosa may bleed easily upon contact with the endoscope.
These inflammatory changes, when captured in endoscopic images, are strong indicators of an active pathological process that could lead to or accompany early ulcer formation. Recognizing these subtle changes is paramount for preventing advanced peptic ulcer complications.
From a symptomatic perspective, early stomach ulcer symptoms are often milder and more intermittent than those of established ulcers. Patients might report:
Mild Epigastric Discomfort: A vague ache or pressure in the upper abdomen rather than sharp pain.
Intermittent Burning Sensation: Not constant, perhaps occurring only after certain meals or during stressful periods.
Occasional Bloating or Fullness: Especially after meals, but not as persistent or severe as with chronic ulcers.
Slight Nausea: Infrequent and not usually leading to vomiting.
Changes in Appetite: A subtle decrease in appetite, or feeling satisfied more quickly than usual.
These subtle ulcer symptoms are often dismissed as indigestion or heartburn, delaying appropriate diagnosis. Early detection through awareness of these symptoms, coupled with diagnostic imaging like endoscopy, is crucial for effective stomach ulcer prevention and ulcer management. Identifying the factors contributing to these early stages, such as H. pylori infection or chronic NSAID use, is also critical for targeted early intervention.
Skin rash Stomach ulcer Images
It is crucial to state upfront that Stomach ulcer images do not typically include skin rashes as a direct symptom. A stomach ulcer is a localized lesion within the gastric lining, and it does not directly cause dermatological manifestations like a rash. However, there are several indirect associations, systemic conditions, or complications related to peptic ulcer disease that might involve skin findings. Therefore, when discussing Skin rash Stomach ulcer Images, one must consider these indirect links rather than direct causation from the ulcer itself. These connections are important for a comprehensive diagnostic approach, especially in cases of complicated ulcer disease or underlying systemic illnesses.
Potential indirect associations between stomach ulcers and skin manifestations include:
Anemia-Related Skin Changes: Chronic gastrointestinal bleeding from an ulcer can lead to iron-deficiency anemia. Signs of anemia visible on the skin include:
Pallor: Generalized paleness of the skin, mucous membranes (gums, conjunctivae), and nail beds. This is a common and visible sign that can be captured in patient photographs.
Koilonychia: Spoon-shaped nails, a sign of severe chronic iron deficiency. While not a rash, it’s a visible skin appendage change.
Angular cheilitis: Cracks and inflammation at the corners of the mouth, also associated with iron deficiency or other nutritional deficiencies from chronic illness.
These are not rashes but are visible skin/mucosal changes indicative of an underlying condition often caused by bleeding ulcers.
Systemic Conditions Predisposing to Ulcers with Skin Involvement: Some rare systemic diseases can cause both ulcers and skin rashes:
Zollinger-Ellison Syndrome (ZES): A condition characterized by gastrinomas (tumors that secrete gastrin), leading to severe, recurrent peptic ulcers and often esophagitis. While ZES itself doesn’t cause a specific rash, it can be associated with Multiple Endocrine Neoplasia type 1 (MEN1), which has its own dermatological signs like angiofibromas or collagenomas, though these are not typical “rashes.” Patients with ZES may also experience flushing due to elevated gastrin levels, which might be perceived as a skin reaction.
Systemic Vasculitis: Conditions like Polyarteritis Nodosa (PAN) or Behcet’s Disease can cause inflammation of blood vessels, leading to ulcers in the gastrointestinal tract and various skin manifestations, including purpura, nodules, ulcers (cutaneous), livedo reticularis, or erythema nodosum. If an ulcer is diagnosed in a patient with one of these systemic vasculitides, then the concurrent skin rash would be related to the underlying vasculitis, not directly the stomach ulcer.
Crohn’s Disease: While primarily affecting the intestines, Crohn’s can cause gastric ulcers and has numerous extraintestinal manifestations, including skin lesions such as erythema nodosum, pyoderma gangrenosum, or aphthous stomatitis.
Mastocytosis/Systemic Mast Cell Activation Syndrome: Can cause peptic ulcers due to histamine release and characteristic skin lesions like urticaria pigmentosa (brownish macules/papules that urticate when rubbed – Darier’s sign) or flushing episodes.
These represent differential diagnoses or comorbidities where ulcers and rashes co-exist.
Medication-Induced Rashes: Many medications used to treat or exacerbate stomach ulcers can cause skin rashes:
NSAIDs: Non-steroidal anti-inflammatory drugs are a common cause of peptic ulcers. They can also cause various drug-induced rashes, including urticaria, maculopapular eruptions, or fixed drug eruptions. The rash is due to the drug, not the ulcer.
Antibiotics: Used in H. pylori eradication therapy, antibiotics (e.g., amoxicillin, clarithromycin) are frequent culprits for allergic skin rashes such as morbilliform rashes or urticaria.
Proton Pump Inhibitors (PPIs): While less common, PPIs can cause drug reactions, including rashes.
Antacids: Rare, but can cause allergic reactions in some individuals.
H. pylori Associated Skin Conditions (Controversial/Indirect): There is some speculative research linking H. pylori infection (a major cause of stomach ulcers) to certain dermatological conditions, although direct causation is not firmly established:
Chronic Urticaria: Some studies suggest a possible link between H. pylori infection and chronic idiopathic urticaria, where eradication of the bacteria may lead to resolution of hives in a subset of patients.
Rosacea: Similar to urticaria, some researchers have explored a connection between H. pylori and rosacea, a chronic inflammatory skin condition characterized by facial redness, papules, and pustules. However, the evidence for a direct causal link is not conclusive.
It is important to emphasize these are H. pylori-associated and not directly ulcer-associated rashes, and the link remains a subject of ongoing research. Therefore, when encountering skin rashes in patients with stomach ulcers, a careful clinical evaluation is necessary to distinguish between incidental findings, drug reactions, underlying systemic diseases, or very rare indirect associations with H. pylori. Skin manifestations are generally not considered a primary symptom in stomach ulcer symptom pictures.
Stomach ulcer Treatment
Stomach ulcer treatment aims to alleviate symptoms, heal the ulcer, prevent complications, and eradicate underlying causes such as H. pylori infection. The approach is typically multi-faceted, combining pharmacotherapy with lifestyle modifications. Understanding the various treatment strategies is crucial for effective ulcer management and ulcer healing.
Pharmacological Treatment:
The cornerstone of stomach ulcer treatment involves medications that reduce stomach acid, protect the gastric lining, and, if necessary, eliminate H. pylori.
1. Proton Pump Inhibitors (PPIs): These are the most effective drugs for acid suppression. They block the proton pumps in the stomach lining, significantly reducing acid production.
Examples: Omeprazole, Esomeprazole, Lansoprazole, Pantoprazole, Rabeprazole.
Duration: Typically prescribed for 4-8 weeks to allow complete ulcer healing.
Role: Essential for healing gastric ulcers and duodenal ulcers, as well as preventing recurrence.
2. H2-Receptor Blockers (H2 blockers): These drugs reduce acid production by blocking histamine’s action on parietal cells.
Examples: Famotidine, Ranitidine (though ranitidine has largely been recalled), Cimetidine, Nizatidine.
Role: Less potent than PPIs but can be used for less severe ulcers or as maintenance therapy for peptic ulcer disease prevention.
3. Antibiotics for H. pylori Eradication: If Helicobacter pylori infection is confirmed, eradication therapy is critical to prevent ulcer recurrence.
Standard Triple Therapy: A PPI + two antibiotics (e.g., Amoxicillin + Clarithromycin, or Metronidazole + Clarithromycin if penicillin allergic) for 10-14 days.
Quadruple Therapy: Often used for resistance or treatment failure, includes a PPI + Bismuth subsalicylate + Metronidazole + Tetracycline for 10-14 days.
Goal: Complete eradication of H. pylori to prevent future gastric ulcers and duodenal ulcers.
4. Antacids: These provide rapid but temporary relief of symptoms by neutralizing existing stomach acid.
Examples: Aluminum hydroxide, Magnesium hydroxide, Calcium carbonate.
Role: Symptomatic relief for ulcer pain, not for healing the ulcer itself.
5. Cytoprotective Agents: These medications protect the stomach lining from acid and promote healing.
Sucralfate: Forms a protective barrier over the ulcer surface.
Misoprostol: A prostaglandin analog that increases mucus and bicarbonate production, particularly useful for NSAID-induced ulcers, though often has side effects.
Bismuth Subsalicylate: Has antimicrobial properties against H. pylori and cytoprotective effects. It’s often included in H. pylori eradication regimens.
Lifestyle and Dietary Modifications:
Lifestyle changes are crucial for supporting ulcer healing and preventing future episodes. These are integral to stomach ulcer prevention.
1. Avoid NSAIDs: If possible, discontinue or reduce the use of non-steroidal anti-inflammatory drugs (e.g., aspirin, ibuprofen, naproxen) as they are a major cause of gastric ulcers. If NSAIDs are essential, protective measures like co-prescribing PPIs or using COX-2 inhibitors may be considered.
2. Smoking Cessation: Smoking impairs ulcer healing and increases the risk of recurrence and complications. Quitting smoking is a critical step in ulcer management.
3. Alcohol Moderation: Excessive alcohol consumption can irritate the stomach lining and impede healing.
4. Stress Management: While stress doesn’t directly cause ulcers, it can exacerbate symptoms and potentially delay healing. Techniques such as meditation, yoga, regular exercise, and adequate sleep are beneficial for ulcer relief.
5. Dietary Adjustments: There isn’t a strict “ulcer diet,” but avoiding foods that trigger symptoms is recommended.
Common Irritants: Spicy foods, acidic foods (citrus, tomatoes), caffeine, chocolate, and carbonated beverages can irritate the stomach.
Eating Habits: Eating smaller, more frequent meals can sometimes be better tolerated than large meals. Avoiding eating close to bedtime can also help prevent nocturnal ulcer pain.
Surgical Treatment:
Surgery for stomach ulcers is rare nowadays due to effective medical therapies but is reserved for ulcer complications or intractable cases.
1. Perforation: An ulcer that has created a hole in the stomach wall is a medical emergency requiring immediate surgical repair (e.g., simple closure with an omental patch).
2. Uncontrolled Bleeding: If endoscopic hemostasis fails to stop severe upper gastrointestinal bleeding, surgery (e.g., oversewing the bleeding vessel) may be necessary.
3. Gastric Outlet Obstruction: Chronic ulcers near the pylorus can cause scarring and narrowing, leading to obstruction. Surgical procedures like pyloroplasty or gastrectomy (partial removal of the stomach) with gastrojejunostomy may be performed to restore patency.
4. Intractability/Recurrence: In very rare cases of recurrent, severe ulcers unresponsive to extensive medical management, surgical options such as vagotomy (cutting the vagus nerve to reduce acid secretion) or partial gastrectomy might be considered for long-term ulcer resolution.
Follow-up and Monitoring:
For gastric ulcers, repeat endoscopy after 6-12 weeks is often recommended to confirm healing and to biopsy the ulcer bed again, especially if there were any suspicious features initially. This is crucial to rule out underlying gastric cancer, which can mimic a benign ulcer. For duodenal ulcers, follow-up endoscopy is usually not necessary if symptoms resolve and H. pylori has been eradicated. Regular monitoring for symptom recurrence and adherence to prescribed medications are vital for maintaining ulcer-free status and preventing future peptic ulcer complications.