For those seeking visual understanding of oral lesions, comprehensive Aphthous stomatitis symptoms pictures can illuminate the characteristic appearance of these common and often painful mouth sores. Understanding the visual presentation through detailed descriptions helps in accurate identification and management of recurrent aphthous stomatitis, distinguishing it from other oral conditions.
Aphthous stomatitis Symptoms Pictures
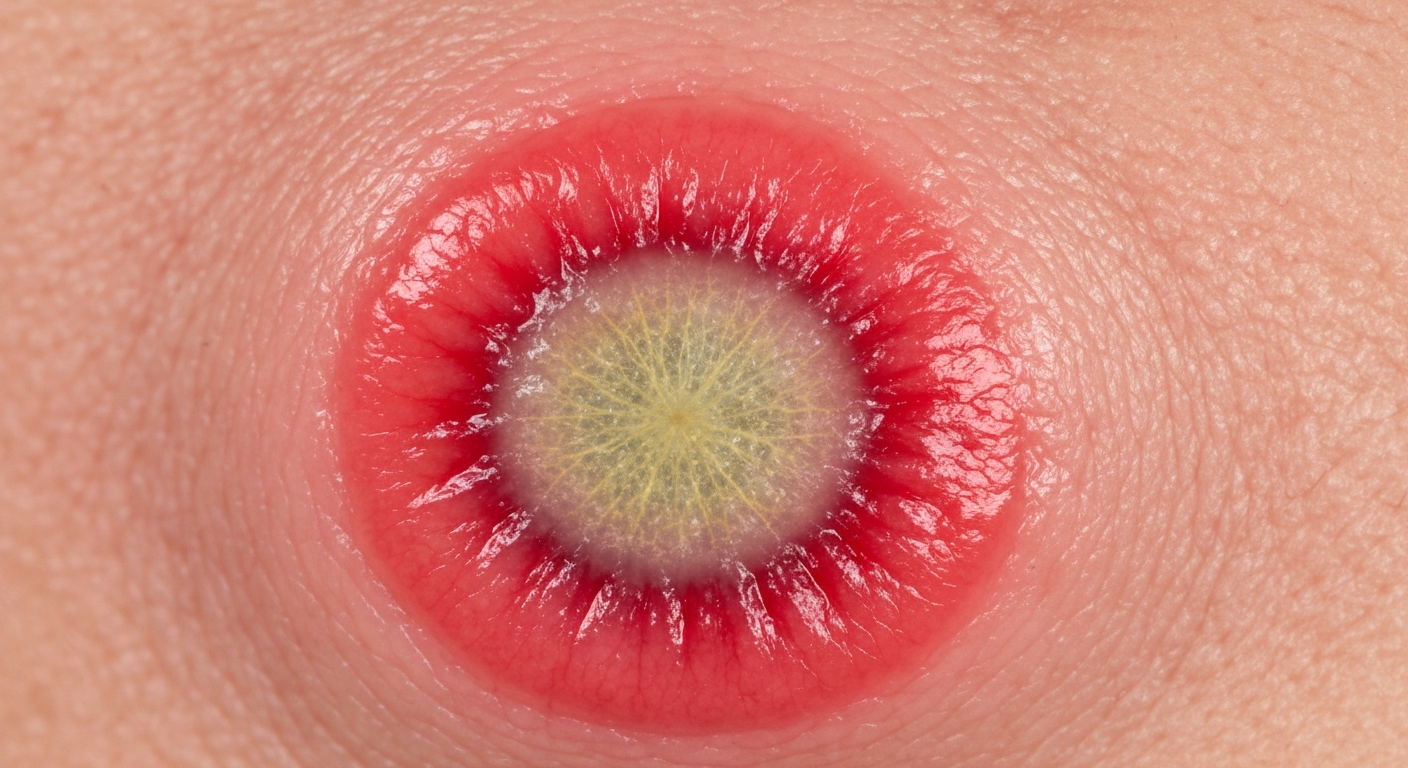
The visual presentation of Aphthous stomatitis is distinct and can be readily recognized in diagnostic images. The primary symptom is the development of one or more painful, round or oval ulcers within the mouth. These oral ulcers typically appear on the movable mucous membranes, such as the inside of the lips, cheeks, the floor of the mouth, the soft palate, and the tongue. They are rarely found on the gums or the hard palate. When observed in Aphthous stomatitis symptoms pictures, the lesions commonly feature a central yellowish-gray base, which is often covered by a fibrinous pseudomembrane, signaling the body’s healing process. This central area is invariably surrounded by a sharply defined, bright red inflammatory halo, highlighting the acute inflammation occurring at the site. The size of these canker sores can vary significantly, from very small pinpoint lesions to larger, more extensive ulcers, impacting the severity of discomfort and functionality. The borders of the lesions are typically smooth and regular, without the raised, indurated edges that might suggest malignancy or other infectious processes. The surrounding tissue, apart from the immediate red halo, usually appears normal and healthy, without widespread inflammation or vesiculation. These distinct visual cues are crucial for accurate identification when reviewing various Aphthous stomatitis symptoms pictures, helping clinicians and patients understand the nature of the condition. The recurrent nature of these mouth sores means that photographic documentation often shows lesions in various stages of healing or new lesions appearing in different locations over time.
Detailed visual characteristics often captured in Aphthous stomatitis symptom images include:
- Central Pseudomembrane: The most identifiable feature is the pale, often yellowish-gray or whitish film covering the ulcer’s base. This fibrinopurulent exudate is a protective layer composed of fibrin, necrotic cellular debris, and inflammatory cells. It gives the ulcer its characteristic color and texture, distinct from the raw, red appearance of some other types of oral wounds.
- Erythematous Halo: A vibrant red ring of inflamed tissue consistently encircles the central pseudomembrane. This distinct halo signifies active inflammation and is a key diagnostic visual cue. The intensity of this redness can vary based on the stage of the ulcer and the individual’s inflammatory response.
- Shape and Margins: Aphthous ulcers are predominantly round or oval. Their margins are typically well-demarcated and regular, meaning they have a smooth, even border where the ulcerated tissue meets the healthy mucosa. Irregular or ragged borders are less common and might prompt investigation for other conditions.
- Location: The vast majority of aphthous lesions are found on non-keratinized oral mucosa. This includes the labial mucosa (inner lips), buccal mucosa (inner cheeks), floor of the mouth, ventral surface of the tongue, and soft palate. Images frequently showcase these lesions in these specific, movable areas.
- Size Variability: Images of Aphthous stomatitis can display a wide range of lesion sizes. Minor aphthae are generally 1-10 mm in diameter, while major aphthae can exceed 1 cm. Herpetiform aphthae appear as clusters of very small, pinpoint ulcers, each typically less than 3 mm.
- Pain Intensity: While not a visual symptom, the severe pain associated with these lesions is a critical aspect that drives patients to seek diagnosis, and descriptions accompanying Aphthous stomatitis symptoms pictures often emphasize this discomfort. The pain is typically proportionate to the size and number of lesions and their location, with ulcers on areas of high movement (e.g., tongue, lips) causing more distress.
- Number of Lesions: Aphthous stomatitis images may show a solitary ulcer or multiple ulcers. Minor aphthae usually present as 1-5 ulcers at a time. Herpetiform aphthae, true to their name, involve numerous (10-100) very small ulcers in clusters. Major aphthae are often solitary or present as a few very large lesions.
- Healing Process: Pictures over time can illustrate the healing phases. Initially, the pseudomembrane may become thicker, and the red halo might fade slightly. As healing progresses, the pseudomembrane detaches, revealing re-epithelialized mucosa underneath. Minor aphthae heal without scarring, while major aphthae can leave a scar due to deeper tissue involvement.
Understanding these visual characteristics through detailed descriptive analysis of Aphthous stomatitis symptoms pictures is essential for distinguishing these common oral ulcers from more serious conditions. The lack of vesicles (blisters) prior to ulceration is a key differentiating factor from herpetic lesions, further aiding in accurate diagnosis of recurrent oral ulcers.
Signs of Aphthous stomatitis Pictures
When examining signs of Aphthous stomatitis in various pictures, it’s crucial to categorize them into the three main clinical types: minor aphthous stomatitis (MiRAS), major aphthous stomatitis (MaRAS), and herpetiform aphthous stomatitis (H RAS). Each type presents with distinct visual signs that are observable in diagnostic images of recurrent aphthae. Minor aphthae, the most common form, typically appear as small, round or oval ulcers, less than 1 cm in diameter. Pictures of MiRAS will show the characteristic yellowish-gray base surrounded by a thin, bright red halo. These lesions are usually shallow and heal without scarring within 7-14 days. They often appear on the non-keratinized mucosa, such as the buccal and labial mucosa, the floor of the mouth, the ventral surface of the tongue, and the soft palate. The integrity of the surrounding tissue, beyond the immediate inflammatory zone, remains intact, which is a consistent visual sign in photographs. The painful nature of these oral lesions is a hallmark, and patients often point to specific spots in pictures where they experience discomfort. The presence of multiple, yet typically few (1-5) such lesions at any given time is a common finding in various signs of Aphthous stomatitis pictures depicting minor aphthae.
Major aphthae, also known as Sutton’s disease or periadenitis mucosa necrotica recurrens, are visually more dramatic and severe. Pictures of MaRAS display much larger ulcers, often exceeding 1 cm in diameter, and can be up to several centimeters across. These lesions are typically deeper and more irregular in shape than minor aphthae, although they still maintain the central pseudomembrane and erythematous halo. The increased depth of these painful mouth sores means that they frequently involve the deeper layers of the oral mucosa, leading to significant tissue destruction. Healing for major aphthae can take weeks to months (3-6 weeks or longer) and often results in scarring, which can be visible in follow-up photographic documentation. Due to their size and depth, major aphthae cause excruciating pain and can significantly impair speech, eating, and drinking. Images might show these larger lesions in areas like the soft palate, tonsillar pillars, or on the tongue, often affecting functionality. The individual presenting with MaRAS usually has only one or a few such lesions at a time. The distinctive deep ulceration and the potential for scar formation differentiate these images from those of minor aphthae.
Herpetiform aphthae (H RAS) are visually distinct as they present as numerous small, pinpoint ulcers, often 1-3 mm in diameter, that frequently coalesce to form larger, irregular ulcers. Despite their name, H RAS are not caused by the herpes virus. Pictures of H RAS showcase clusters of these tiny lesions, resembling a widespread eruption. There can be dozens, or even hundreds, of these small oral ulcerations present simultaneously. These clusters are often seen on the tongue, soft palate, or any other oral mucosal site. The individual ulcers within the cluster still feature the characteristic gray-white base and red halo. While each lesion is small, their sheer number and tendency to merge can make H RAS incredibly painful and debilitating. They heal without scarring, typically within 7-14 days. The unique “cluster” or “field” appearance of multiple small ulcers distinguishes H RAS from both minor and major forms when viewing Aphthous stomatitis pictures. The visual complexity of H RAS, with its numerous small lesions, can sometimes be mistaken for primary herpetic gingivostomatitis, but the key differentiating factor in imagery is the absence of a vesicular (blister) stage in aphthous stomatitis; lesions appear as ulcers from the outset.
Additional observable signs in Aphthous stomatitis pictures, beyond the ulcer morphology, include:
- Location on Movable Mucosa: Consistent observation in images shows lesions primarily on non-keratinized, movable parts of the oral cavity. This specificity is a diagnostic clue, as lesions on keratinized mucosa (attached gingiva, hard palate) are less typical for Aphthous stomatitis.
- Absence of Vesicles: A critical differentiating sign. Unlike herpetic lesions which begin as fluid-filled blisters (vesicles) that rupture to form ulcers, Aphthous stomatitis lesions present directly as ulcers. This lack of a preceding vesicular stage is a consistent visual finding.
- Healthy Surrounding Mucosa: Outside the immediate red halo, the oral mucosa typically appears healthy and free from widespread inflammation, erythema, or other lesions. This localized inflammation is a strong indicator.
- Recurrence Patterns: While not a single visual sign, a series of Aphthous stomatitis pictures over time might demonstrate the pattern of recurrence, with lesions appearing, healing, and then new ones emerging in different locations. This historical photographic evidence supports the diagnosis of recurrent aphthous ulceration.
- Patient Demographics (Implied): Though not directly visual, the context of who is pictured (e.g., adolescent, young adult) can hint at common demographics for RAS, as it frequently affects individuals in these age groups.
- Impact on Functionality: In severe cases, particularly with major aphthae, images might indirectly convey the functional impairment, such as difficulty opening the mouth fully or visible signs of discomfort during oral movements, though this is inferred rather than directly observed as a lesion characteristic.
- Lack of Systemic Signs (Typically): Pure Aphthous stomatitis does not typically present with fever, lymphadenopathy, or malaise as primary signs. If such systemic signs are present alongside oral aphthae, it usually indicates an underlying systemic condition, which would prompt further investigation beyond simple Aphthous stomatitis pictures.
- Healing Without Scarring (MiRAS, HRAS): For minor and herpetiform types, serial photographs would demonstrate complete resolution of the mucosa without any lasting marks. This is a positive prognostic sign.
Each of these visual signs, when carefully analyzed in Aphthous stomatitis pictures, contributes significantly to the accurate identification and classification of these common, yet often debilitating, oral conditions.
Early Aphthous stomatitis Photos
Early Aphthous stomatitis photos capture the initial, often subtle, visual cues that precede the fully formed ulcer. These images are invaluable for understanding the prodromal stage, a period of sensation before any overt lesion appears, and the very first visible signs of an impending oral ulcer. The earliest visible manifestation, typically lasting for a few hours to a a day or two, can be seen as a small, localized area of redness or erythema on the oral mucosa. This erythema may be accompanied by a slight swelling or induration, forming a small papule. In early Aphthous stomatitis pictures, this erythematous macule or papule is usually quite small, often just a few millimeters in diameter, but it is characteristically tender and sensitive to touch or irritation. Patients often report a tingling, burning, or itching sensation in this precise spot even before any visible lesion develops, providing an important subjective symptom that aligns with these early photographic findings. This initial red spot is the harbinger of the impending ulceration and represents the localized inflammatory response beginning to take hold in the tissue. The surrounding mucosa generally appears healthy and unaffected at this very early stage, with the inflammation strictly confined to the nascent lesion area, a key visual observation in initial aphthous lesion images.
As the condition progresses from this initial erythematous stage, the surface of the papule rapidly breaks down, leading to the formation of an ulcer. This process can be quite rapid, often occurring within 24-48 hours of the first visible sign. Early Aphthous stomatitis photos will then show a small, shallow ulcer, sometimes barely visible, with the very beginnings of the characteristic yellowish-gray fibrinopurulent base. The red halo of inflammation is also present from the outset, intensifying as the ulcer matures. The transition from an intact mucosal surface to an ulcer is a rapid inflammatory event. This rapid evolution from a subtle red spot to a definitive ulcer differentiates aphthous lesions from conditions that might have a longer prodromal blister stage. Understanding these initial visual presentations through carefully documented first signs of canker sores photos is vital for early intervention and patient education, helping individuals identify the onset of an episode and potentially manage symptoms sooner. The localized nature of the early redness and the subsequent quick progression to ulceration are consistent visual patterns observed in various photographic records.
Specific visual markers identifiable in early Aphthous stomatitis images:
- Localized Erythema: The very first observable sign is often a small, distinct patch of redness, usually no more than a few millimeters wide. This initial red spot indicates localized inflammation before tissue breakdown.
- Subtle Swelling/Induration: Accompanying the redness, there may be a slight elevation or firmness to the touch in the affected area, representing an early inflammatory infiltrate. This forms a small, tender papule.
- Absence of Vesicles or Bullae: Crucially, early Aphthous stomatitis photos will not show any fluid-filled blisters (vesicles or bullae). The lesion progresses directly from a red macule/papule to an ulcer, distinguishing it from herpetic infections.
- Sharp Demarcation: Even in its nascent stage, the early lesion typically has a relatively well-defined border, separating the inflamed area from the healthy surrounding mucosa.
- Rapid Ulceration: Subsequent photos taken within a day or two of the initial redness will demonstrate the breakdown of the mucosal surface, revealing a small, shallow ulcer. This rapid transition is a key characteristic.
- Beginning of Pseudomembrane Formation: As ulceration occurs, a thin, whitish or yellowish film (fibrinous exudate) starts to cover the base of the lesion. This is the precursor to the more prominent pseudomembrane seen in mature ulcers.
- Developing Inflammatory Halo: The red halo, characteristic of the mature aphthous ulcer, begins to form around the nascent ulcer, often appearing as a slightly intensified ring of redness.
- Focal Presentation: Early images almost always show a singular focal lesion, even if multiple ulcers are to develop eventually. The inflammatory process typically begins at discrete points.
- Intense Sensitivity/Pain (Implied): While not directly visual, the localized discomfort reported by patients at this stage is a strong indicator and correlates with the visual signs of early inflammation and tissue damage.
Recognizing these distinct features in early lesion photographs is paramount for understanding the pathogenesis of Aphthous stomatitis and for distinguishing it from other conditions presenting with similar initial oral mucosal changes. The absence of a blister stage is a consistently important diagnostic point when reviewing all stages of aphthous disease, including these initial presentations.
Skin rash Aphthous stomatitis Images
It is critical to clarify that typical, uncomplicated Aphthous stomatitis (recurrent aphthous stomatitis, RAS) is primarily an oral mucosal condition and does not cause a “skin rash” on the external skin surfaces of the body. When Aphthous stomatitis pictures are discussed in the context of a skin rash, it usually refers to a broader differential diagnosis, where oral aphthous-like ulcers are a feature of a systemic disease that *also* manifests with dermatological signs. Therefore, images under this heading would typically depict individuals with recurrent oral aphthous ulcers alongside various extraoral skin manifestations, indicating an underlying systemic condition rather than pure RAS. These associated conditions are significant because they often present with similar painful oral lesions, making accurate diagnosis crucial. The distinction between localized oral aphthae and oral aphthae as part of a multi-systemic disorder is vital for proper management and treatment planning, moving beyond simple symptomatic relief to addressing the underlying systemic issue. If oral aphthae images are accompanied by photos of skin lesions, it immediately suggests the need for a comprehensive medical evaluation to identify the associated systemic disease. Such presentations broaden the scope from simple Aphthous stomatitis symptoms pictures to a more complex diagnostic landscape.
Conditions that present with aphthous-like oral ulcers and various forms of skin rashes or lesions include:
- Behçet’s Disease: This is a chronic, relapsing, multi-system inflammatory disorder characterized by recurrent oral aphthous ulcers, recurrent genital ulcers, and various ocular lesions. When reviewing skin rash Aphthous stomatitis images in this context, one might see:
- Erythema Nodosum-like Lesions: These appear as tender, red, subcutaneous nodules, typically on the lower legs, but can occur elsewhere. In pictures, they look like raised, painful lumps under the skin.
- Pseudofolliculitis/Papulopustular Lesions: Resembling acne, these are small, red bumps (papules) or pus-filled bumps (pustules) that can be widespread, particularly on the trunk and limbs.
- Acneiform Nodules: More severe, cyst-like acne lesions.
- Vascular Lesions: Reticular patterns (livedo reticularis) or superficial thrombophlebitis (inflamed veins).
- Pathergy Phenomenon: A characteristic non-specific skin hyperreactivity where a sterile papule or pustule develops 24-48 hours after a skin prick or minor trauma. Pictures might show such lesions developing after a needle stick.
In images of Behçet’s disease, the oral aphthous ulcers themselves often resemble major aphthae, being large, deep, and painful, alongside these varied skin findings, providing a comprehensive visual picture of this complex disease.
- Inflammatory Bowel Disease (IBD) – Crohn’s Disease and Ulcerative Colitis: Oral aphthous-like ulcers are common extraintestinal manifestations of IBD. If Aphthous stomatitis images are presented with associated skin rashes, these could include:
- Erythema Nodosum: Identical to those seen in Behçet’s disease, presenting as tender red nodules on the shins.
- Pyoderma Gangrenosum: A severe, rare condition characterized by rapidly enlarging, painful ulcerative lesions with undermined, violaceous borders. Pictures would show deep, necrotic ulcers, often on the legs, sometimes elsewhere.
- Sweet’s Syndrome (Acute Febrile Neutrophilic Dermatosis): Characterized by the sudden onset of fever, leukocytosis, and tender, erythematous plaques that may have a pseudovesicular appearance. Images show bright red, raised plaques.
- Metastatic Crohn’s Disease: Skin lesions that show granulomatous inflammation microscopically and are contiguous with the gastrointestinal tract, or occur at sites distant from the bowel but still histologically similar.
The oral ulcers in IBD can be indistinguishable from common recurrent aphthae, but the presence of concurrent skin lesions or gastrointestinal symptoms necessitates a broader diagnostic perspective when interpreting the images.
- Celiac Disease: While less directly associated with a “rash” in the classical sense, celiac disease can present with recurrent aphthous stomatitis and is associated with dermatitis herpetiformis.
- Dermatitis Herpetiformis: This is an intensely itchy, chronic papulovesicular (small bumps and blisters) skin eruption, typically symmetrical on the elbows, knees, buttocks, and scalp. Pictures would show grouped vesicles on erythematous bases. The association with oral aphthae is well-documented.
- Systemic Lupus Erythematosus (SLE): This autoimmune disease can cause oral ulcers, which may be aphthous-like, alongside a wide array of skin manifestations.
- Malar Rash (Butterfly Rash): A classic sign, appearing as a red rash over the cheeks and bridge of the nose, sparing the nasolabial folds. Images show a distinct butterfly-shaped erythema.
- Discoid Lupus Erythematosus: Chronic skin lesions that are red, raised, scaly, and can cause scarring and hair loss.
- Subacute Cutaneous Lupus Erythematosus: Non-scarring, non-pruritic, annular (ring-shaped) or papulosquamous (scaly bumps) lesions, often on sun-exposed areas.
The oral ulcers in SLE can be varied, including aphthous-like types, making the co-occurrence with characteristic lupus skin rashes a crucial diagnostic visual cue in comprehensive patient images.
- Reiter’s Syndrome (Reactive Arthritis): This triad of arthritis, urethritis, and conjunctivitis can also include oral ulcers and skin lesions.
- Keratoderma Blennorrhagicum: Psoriasis-like lesions, often waxy, yellow-brown, hyperkeratotic papules and plaques, especially on the palms and soles. Pictures show distinctive scaly, sometimes pustular, skin changes.
- Circinate Balanitis: Penile lesions, often appearing as shallow erosions.
- Nutritional Deficiencies: While not a systemic disease causing a “rash” directly, deficiencies in iron, folate, vitamin B12, or zinc are linked to recurrent aphthous stomatitis. Severe deficiencies can sometimes manifest with other non-specific skin changes (e.g., pallor from anemia), which might be subtly visible in clinical images.
Therefore, when analyzing “skin rash Aphthous stomatitis images,” it’s about looking for patterns of multi-system involvement where oral aphthae are just one component of a larger clinical picture. The oral lesions themselves may appear identical to routine aphthae, but the accompanying dermatological findings, such as those described above, point towards an underlying systemic pathology requiring a distinct diagnostic and therapeutic approach. These situations demand careful medical investigation to move beyond mere symptomatic treatment of the mouth ulcers to addressing the root cause of the widespread symptoms.
Aphthous stomatitis Treatment
Treatment for Aphthous stomatitis primarily focuses on pain relief, reducing inflammation, accelerating healing, and preventing recurrence. Since there is no definitive cure for recurrent aphthous stomatitis, management strategies are typically symptomatic and supportive. The choice of treatment often depends on the severity, frequency, and impact of the oral ulcers on the patient’s quality of life. For minor and infrequent aphthae, over-the-counter remedies and simple home care might suffice. However, more severe or persistent cases, such as major aphthae or herpetiform aphthae, often require prescription medications and a more aggressive therapeutic approach. The aim is to make the episodes less debilitating and to shorten the duration of each ulcer. Understanding the different treatment modalities is crucial for patients experiencing recurrent canker sores, as timely intervention can significantly improve comfort and functional ability. The range of treatments for Aphthous stomatitis is broad, encompassing topical agents, systemic medications, and various adjunctive therapies designed to alleviate the painful symptoms and foster a quicker resolution of the lesions.
Detailed treatment options for Aphthous stomatitis include:
- Topical Corticosteroids: These are the cornerstone of treatment for reducing inflammation and pain. They come in various forms such as gels, creams, ointments, and rinses.
- Triamcinolone Acetonide (0.1%): Often prescribed in an adhesive paste (e.g., Orabase) to provide a protective barrier and allow the steroid to act locally. Applied directly to the lesion 2-4 times daily.
- Fluocinonide (0.05%) Gel/Ointment: A more potent steroid for more severe or larger lesions.
- Clobetasol Propionate (0.05%) Gel/Ointment: A very potent steroid, typically reserved for severe cases under careful supervision due to potential for local side effects with prolonged use.
- Dexamethasone Elixir (0.5 mg/5 mL): Used as a rinse for multiple or hard-to-reach lesions. Patients rinse and spit, or rinse and swallow depending on physician instructions.
Topical steroids should be applied after meals and at bedtime to maximize contact time with the lesion, aiding in the reduction of inflammation and pain associated with aphthous ulcers.
- Topical Anesthetics/Analgesics: Provide temporary pain relief, especially before eating or speaking.
- Lidocaine Viscous (2%): A powerful local anesthetic that can be applied directly to the ulcer or used as a rinse. It numbs the area, allowing for comfortable eating and drinking. Caution is advised to avoid systemic absorption, especially in children.
- Benzocaine (20%) Gels/Liquids: Over-the-counter options for temporary pain relief.
- Dyclonine Hydrochloride (0.5% or 1%) Rinse: Another effective topical anesthetic for widespread pain.
These agents are particularly useful for managing the severe discomfort caused by painful mouth sores.
- Antimicrobial Rinses: While not directly treating the aphthae, they can prevent secondary infection and keep the mouth clean, promoting healing.
- Chlorhexidine Gluconate (0.12%) Rinse: Reduces oral bacterial load and can promote healing by creating a cleaner environment. Used twice daily.
- Tetracycline Suspension: Although an antibiotic, it is thought to act more through its anti-inflammatory properties when used as a rinse for aphthous ulcers. It can be made by dissolving tetracycline capsules in water and used as a rinse and spit.
These rinses contribute to overall oral hygiene, which is beneficial for managing recurrent oral ulcers.
- Systemic Medications: Reserved for severe, recalcitrant, or frequently recurring cases, particularly major aphthae or when topical treatments fail.
- Systemic Corticosteroids (e.g., Prednisone): Used for short courses to gain control over severe outbreaks. Due to side effects, long-term use is generally avoided.
- Immunomodulators/Immunosuppressants (e.g., Colchicine, Thalidomide, Pentoxifylline, Azathioprine): For extremely severe or refractory cases, particularly when associated with systemic diseases like Behçet’s. These medications require careful monitoring due to their significant side effect profiles.
- Dapsone: An anti-inflammatory and immunomodulatory drug that may be used in some resistant cases.
These systemic options target the underlying inflammatory response responsible for the severe presentation of aphthous lesions.
- Adjunctive Therapies and Lifestyle Modifications:
- Nutritional Supplementation: If deficiencies are identified (e.g., iron, folate, vitamin B12, zinc), supplementation can reduce the frequency and severity of outbreaks.
- Dietary Modification: Avoiding irritating foods (acidic, spicy, salty, abrasive) can prevent exacerbation of pain and potentially reduce recurrence triggers for mouth ulcer symptoms.
- Stress Reduction: Stress is a known trigger for many individuals. Techniques like meditation, yoga, or counseling can be beneficial.
- Avoidance of Trauma: Being mindful of oral trauma from brushing, dental work, or biting can help, as minor injuries can trigger aphthae.
- Sodium Lauryl Sulfate (SLS)-Free Toothpaste: Some individuals find that toothpastes containing SLS can trigger or worsen aphthae. Switching to an SLS-free option may be helpful.
- Silver Nitrate/Debacterol: Chemical cauterization can provide immediate pain relief and accelerate healing for individual, larger lesions, but it must be applied by a healthcare professional and can be painful during application.
- Low-Level Laser Therapy (LLLT): Some studies suggest that LLLT can reduce pain and accelerate healing of aphthous ulcers, with no reported side effects.
These supportive measures are crucial for comprehensive management and improving the patient’s experience with recurrent aphthous stomatitis. A multi-faceted approach combining medication with lifestyle adjustments typically yields the best results for long-term control of this chronic condition.