Skin changes can be concerning, and understanding the visual presentation of conditions like Basal cell carcinoma is crucial for early detection. This article provides a detailed visual guide to Basal cell carcinoma of the skin symptoms pictures, helping to identify potential signs of this common skin cancer. Recognizing these characteristic features is an important step in prompt diagnosis and effective management.
Basal cell carcinoma of the skin Symptoms Pictures
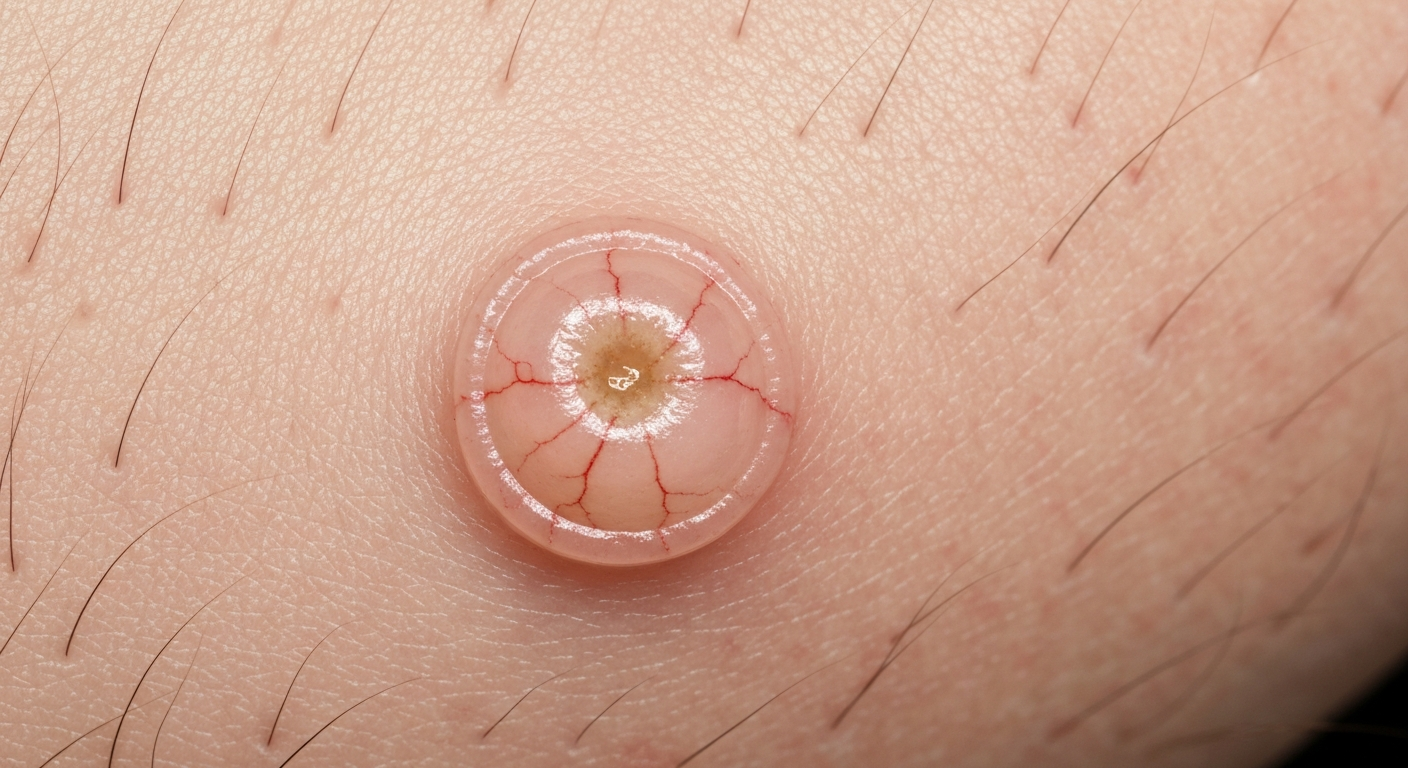
Basal cell carcinoma (BCC) is the most common form of skin cancer, and its visual presentation can vary significantly, making comprehensive understanding of Basal cell carcinoma symptoms critical for accurate identification. When viewing Basal cell carcinoma of the skin symptoms pictures, several key features frequently stand out, providing vital clues for dermatologists and patients alike. A hallmark visual characteristic of many BCCs is a pearly or translucent bump. This small, often flesh-colored, pink, or reddish growth often exhibits a waxy quality, catching light in a distinctive manner. On closer inspection, particularly in magnified images, fine blood vessels, known as telangiectasias, may be visible within or surrounding the lesion, appearing like tiny red threads snaking across the surface. These vessels are a common, though not exclusive, feature of BCC lesions and are often depicted clearly in detailed Basal cell carcinoma images.
Another prevalent symptom depicted in Basal cell carcinoma photos is a central indentation or ulceration. As the lesion grows, the center can break down, forming an open sore or a crusted area that may bleed easily, heal, and then reopen. This persistent non-healing wound is a red flag for potential skin malignancy. Surrounding this ulceration, a characteristic rolled border is frequently observed. This border appears slightly raised and firm, often maintaining the pearly or translucent quality seen in the initial bump. The combination of central ulceration with a rolled, pearly border is a classic visual descriptor of nodular Basal cell carcinoma, one of the most common subtypes, and is frequently highlighted in medical Basal cell carcinoma of the skin symptoms pictures to educate on typical presentations.
Furthermore, Basal cell carcinoma can also present as a flat, firm, pale, or yellow area that might resemble a scar. This particular presentation, often referred to as morpheafrom or sclerosing BCC, is characterized by its ill-defined borders and a harder texture compared to surrounding skin. Unlike the more obvious nodular type, these lesions often lack the distinct pearly appearance and prominent telangiectasias, making them more challenging to identify visually without the aid of high-resolution images that emphasize subtle textural changes and discoloration. In Basal cell carcinoma of the skin symptoms pictures, these scar-like lesions may appear as an irregular patch of skin with a subtly altered texture, often slightly depressed, and are less likely to bleed spontaneously unless subjected to trauma. These variants underscore the importance of observing not just color and shape, but also texture and firmness when evaluating potential skin cancer signs.
Some Basal cell carcinomas can also manifest as dark or pigmented lesions. These pigmented BCCs can be confused with moles or even melanoma due to their brown, black, or blue coloration. However, distinguishing features often observable in high-quality Basal cell carcinoma photos include the typical pearly border, rolled edges, and telangiectasias visible even through the pigmentation. The distribution of pigment in BCCs tends to be more irregular or patchy compared to benign moles, and a closer look might reveal areas where the classic pearly texture is still present. This diverse range of visual characteristics emphasizes the need for careful examination of all suspicious skin lesions and highlights why a collection of varied Basal cell carcinoma of the skin symptoms pictures is invaluable for diagnostic training and patient awareness. The persistent growth, non-healing nature, and specific textural qualities are often more indicative than color alone, especially when considering the broad spectrum of Basal cell carcinoma presentations captured in visual symptom guides.
In addition to the aforementioned characteristics, Basal cell carcinoma may also appear as shiny bumps or nodules. These growths can range in size from very small, almost pinhead-sized, to much larger lesions that spread across significant areas of the skin. The shininess is directly related to the pearly translucence, often becoming more pronounced as the lesion enlarges. The surface may be smooth or slightly irregular, and in many instances, patients report that these lesions are asymptomatic in their early stages, lacking pain or itching, which can contribute to delayed detection. However, as the tumor progresses, it may become itchy, bleed with minor trauma, or develop a crust that repeatedly falls off and reforms, leaving behind a persistent sore. These progression patterns are crucial to recognize and are often documented through sequential Basal cell carcinoma of the skin symptoms pictures showing the evolution of the lesion over time.
Another less common but visually distinct presentation is the superficial Basal cell carcinoma. This type often appears as a flat, reddish patch of skin, sometimes with a slightly scaly or crusty surface, commonly found on the trunk and extremities. In Basal cell carcinoma of the skin symptoms pictures, these lesions can strikingly resemble patches of eczema, psoriasis, or chronic dermatitis. However, key differentiating features, if carefully observed, include a subtle, raised, thread-like border which may be pearly, and a tendency for the lesion to slowly enlarge over months or years. Unlike inflammatory skin conditions, superficial BCCs typically do not resolve with standard topical treatments and often persist or even ulcerate over time. This particular presentation underscores the importance of persistent skin lesions being evaluated by a dermatologist, especially when they do not respond to conventional therapies, as visually highlighted in diagnostic Basal cell carcinoma images that contrast it with benign conditions.
The location of Basal cell carcinoma lesions is also an important aspect frequently emphasized in symptom guides and image collections. While BCCs can occur anywhere on the body, they are most commonly found on sun-exposed areas. This includes the face, especially the nose, forehead, cheeks, and around the eyes, as well as the ears, neck, scalp, shoulders, and back. Basal cell carcinoma of the skin symptoms pictures often feature lesions in these prominent locations, illustrating the strong association with ultraviolet (UV) radiation exposure. Lesions on the face, due to cosmetic and functional concerns, require particularly careful visual assessment and prompt intervention. Understanding these characteristic locations further aids in the initial recognition of suspicious growths, prompting individuals to seek medical advice for any persistent or changing skin anomaly that aligns with the visual cues of Basal cell carcinoma.
Signs of Basal cell carcinoma of the skin Pictures
Delving deeper into the specific signs visible in Basal cell carcinoma of the skin pictures reveals the diverse morphology of this common skin cancer. Each subtype of BCC presents with distinct visual cues that are critical for differential diagnosis. The most prevalent type, Nodular Basal cell carcinoma, is frequently depicted as a dome-shaped, flesh-colored, pink, or red papule or nodule. In high-resolution images, its hallmark pearly border and often central depression or ulceration are unmistakable. The pearly luster is due to the translucency of the tumor cells, allowing light to scatter uniquely. Furthermore, the presence of numerous fine, branching blood vessels (telangiectasias) on the surface is a common and highly characteristic sign captured in detailed Nodular Basal cell carcinoma photos, distinguishing it from benign moles or cysts. These vessels are dilated capillaries that proliferate within the tumor, contributing to its reddish hue and making it prone to bleeding with minimal trauma.
Superficial Basal cell carcinoma, another common subtype, offers a different set of visual signs. In Basal cell carcinoma of the skin pictures, it typically appears as a flat, red or pink patch, often slightly scaly or crusty, which can be easily mistaken for eczema or psoriasis. However, close examination, particularly in well-lit images, may reveal a subtle, thread-like, raised, and often pearly border that surrounds the patch, a key differentiator from inflammatory dermatoses. These lesions often grow slowly, expanding outwards, and may show areas of central clearing or atrophy while the border continues to advance. The subtle pearliness of the border is a crucial sign often emphasized in diagnostic image sets, as it helps distinguish this BCC subtype from other erythematous skin conditions. Superficial BCCs are commonly found on the trunk and extremities, making their visual recognition in these areas particularly important for early detection and treatment.
The visual signs of Morpheafrom (Sclerosing) Basal cell carcinoma are perhaps the most challenging to identify from Basal cell carcinoma photos due to their subtle nature. These lesions often present as a flat, indurated, waxy, scar-like plaque that can be pale yellow or white. They typically lack the prominent pearly border and telangiectasias seen in nodular BCC. In images, the key visual signs are a subtle depression, a firm texture that is palpable if one could touch the lesion, and ill-defined borders that blend almost imperceptibly with the surrounding skin. This infiltrative growth pattern makes morpheafrom BCC particularly aggressive locally, despite its innocuous appearance. The lack of classic BCC features often leads to delayed diagnosis, underscoring the importance of comparing suspected lesions with a wide array of Basal cell carcinoma of the skin symptoms pictures, especially those highlighting less typical presentations. The visual cue of a persistent, unexplained scar-like lesion should always raise suspicion.
Pigmented Basal cell carcinoma represents another variant whose visual signs can be misleading. In Basal cell carcinoma of the skin pictures, these lesions exhibit shades of brown, black, or blue, due to melanin deposition within the tumor. While resembling moles or melanoma, careful inspection of images often reveals classic BCC features like a pearly border, rolled edges, and telangiectasias, which might be visible even amidst the pigmentation. The pigment can be irregularly distributed, sometimes appearing as dark flecks or streaks within an otherwise typical nodular or superficial BCC structure. These visual characteristics, when highlighted in comparative Basal cell carcinoma images, help differentiate pigmented BCC from other pigmented lesions. The presence of a shiny or pearly component alongside irregular pigmentation is a strong indicator of pigmented BCC, guiding clinicians toward appropriate diagnostic steps.
Finally, the visual signs of Basosquamous Basal cell carcinoma, a rarer and more aggressive subtype, can incorporate features of both BCC and squamous cell carcinoma. In pictures, these lesions might present with a more inflamed, crusted, or ulcerated appearance, possibly larger and faster-growing than typical BCCs. They may have less of the classic pearly sheen and more of a reddish, scaly, or keratotic component. The visual recognition of this subtype often relies on a combination of BCC-like features (e.g., rolled border, some translucency) with more aggressive, infiltrative growth patterns and a less well-defined lesion margin, making definitive diagnosis challenging without biopsy. Comprehensive collections of Basal cell carcinoma of the skin symptoms pictures often include examples of these rarer variants to ensure that all potential visual manifestations are covered, providing a robust visual dictionary for clinical evaluation.
The progression of these visual signs over time is also a critical diagnostic clue often illustrated through sequential Basal cell carcinoma of the skin symptoms pictures. A lesion that initially appears as a small, inconspicuous bump may gradually enlarge, develop a central ulceration, or show increasing prominence of its pearly border and telangiectasias. Any persistent lesion that grows, changes color, bleeds, or fails to heal over several weeks should be carefully evaluated. The visual evolution of a suspicious skin lesion is a powerful indicator, and a photographic history of the lesion can be highly valuable in diagnosing Basal cell carcinoma. The continuous monitoring for these subtle and overt changes forms the cornerstone of effective early detection strategies.
Other less common but visually distinct signs include the presence of cystic Basal cell carcinoma, which may appear as a translucent, fluid-filled nodule, sometimes with a bluish tint, especially when larger. These lesions are typically soft to the touch, and their cystic nature can be visually inferred from the smooth, often dome-shaped, surface with a distinct boundary. Another variant, infiltrative Basal cell carcinoma, often presents similarly to morpheafrom BCC with ill-defined borders and a scar-like appearance, but might show more aggressive local invasion. In images, the visual difference lies in the subtle textural variations and the extent of indistinctness at the lesion’s periphery. These varied visual signs underscore the complex nature of Basal cell carcinoma and highlight the indispensable role of a comprehensive visual guide to its many manifestations for both medical professionals and the general public concerned about unusual skin growths.
Early Basal cell carcinoma of the skin Photos
Detecting Basal cell carcinoma in its earliest stages is paramount for successful treatment and prevention of extensive tissue damage. Early Basal cell carcinoma photos often reveal very subtle changes that can be easily overlooked or mistaken for benign skin conditions, emphasizing the need for heightened awareness and careful self-examination. One of the most common early presentations is a small, shiny bump, often described as pearly or translucent, which may resemble a simple pimple or an insect bite that does not resolve. Unlike a typical pimple, this early BCC lesion will persist for weeks or months, often without pain or tenderness. In detailed early Basal cell carcinoma images, this bump may be flesh-colored, pink, red, or even slightly brownish, making its initial identification challenging against varied skin tones. The subtle pearliness, however, is a key visual differentiator, though it might not be immediately obvious without close inspection.
Another common early sign captured in Basal cell carcinoma photos is a small, persistent sore that bleeds easily, crusts over, and then reopens. This non-healing characteristic is a critical early warning sign. Initially, it might appear as a tiny scratch or a cut that simply won’t heal completely, repeatedly forming a scab that falls off only for the lesion to bleed again. These early ulcerations are typically small, perhaps just a few millimeters in diameter, but their persistence over several weeks is highly suspicious. In Basal cell carcinoma of the skin symptoms pictures, such early lesions might show minimal surrounding inflammation, but the central erosion or crusting remains a prominent feature, indicating a disruption of the skin’s normal healing processes.
Early Basal cell carcinoma can also manifest as a reddish patch or irritated area, particularly common in the superficial subtype. In early Basal cell carcinoma photos, this patch might resemble eczema, psoriasis, or a persistent rash. It can be slightly scaly, itchy, or even mildly painful, but it generally does not respond to over-the-counter creams or topical steroids designed for inflammatory conditions. A distinguishing feature, often subtle in early images, is a slightly raised, thread-like border that may have a pearly sheen. This border is often the first visual cue to differentiate it from benign rashes. The presence of such a persistent, slowly enlarging patch, especially on sun-exposed areas like the trunk or extremities, should prompt further investigation. These images help train the eye to spot the nuanced differences between a common rash and an evolving skin malignancy.
A less common but important early sign is a scar-like area that appears without a preceding injury. This visual symptom is characteristic of morpheafrom BCC in its incipient stages. In early Basal cell carcinoma photos, this might appear as a flat, waxy, or firm white-to-yellowish patch of skin with poorly defined borders. It might be slightly depressed below the surrounding skin and lacks the obvious pearly appearance or telangiectasias of nodular BCC. The texture is key here – a firm, often subtly indurated feel is clinically significant. For a patient, the visual cue is an unexplainable new “scar” that slowly develops and persists. Recognizing these subtle textural changes in early Basal cell carcinoma images is crucial, as morpheafrom BCC can be more infiltrative and aggressive despite its benign appearance.
Another early manifestation highlighted in Basal cell carcinoma images is a small, pink or reddish growth with a slightly raised, translucent border. This could be the nascent stage of a nodular BCC, before significant ulceration or prominent telangiectasias develop. The translucency gives it a distinctive glow when light hits it, even if the bump itself is very small. Sometimes, a tiny, almost imperceptible dimple might be present in the center. These small, persistent growths, especially when found on the face, neck, or other sun-exposed areas, are important to monitor. The presence of even one or two minute, thread-like blood vessels might be visible with magnification in very early photos, offering an additional diagnostic clue for suspicious skin lesions.
The absence of typical symptoms like pain, itching, or rapid growth can also be an early sign in itself, contributing to delayed diagnosis. Many early Basal cell carcinoma lesions are asymptomatic. Patients might only notice a persistent “blemish” or a spot that just doesn’t look right. Therefore, systematic self-skin examination, coupled with awareness of what to look for in early Basal cell carcinoma photos, is essential. Any new growth, sore that doesn’t heal, or change in an existing lesion, regardless of its size or symptoms, warrants professional evaluation. The key takeaway from reviewing early Basal cell carcinoma of the skin symptoms pictures is to prioritize persistence and atypical appearance over the presence of pain or rapid change, as BCC often presents insidiously.
An often overlooked early sign that can be depicted in Basal cell carcinoma images is a crusted or scaly area that does not heal. This might appear as a small, rough patch, similar to actinic keratosis, but it persists beyond the typical timeframe for such sun-damage related lesions to flake off and resolve. Unlike a temporary scab, the underlying lesion remains, and the crusting repeatedly forms. The borders might be indistinct, but upon careful observation, a subtle raised edge could be present. This type of presentation often indicates an early superficial BCC, especially when located on the trunk or limbs. The educational value of such Basal cell carcinoma of the skin symptoms pictures is immense, as they teach individuals to recognize the subtle, non-healing characteristics that distinguish early malignancy from benign skin conditions.
Skin rash Basal cell carcinoma of the skin Images
When reviewing skin rash Basal cell carcinoma of the skin images, the focus often shifts to the superficial subtype, which has a notorious ability to mimic common inflammatory skin conditions. This chameleon-like presentation makes it particularly challenging to diagnose without a keen eye and often necessitates biopsy. Superficial Basal cell carcinoma frequently appears as a red or pink patch, often with a subtle scaly or crusty surface, strikingly similar to patches of eczema, psoriasis, or tinea (ringworm). However, critical differentiating features are frequently visible in diagnostic Basal cell carcinoma images, guiding accurate identification.
One of the most important visual cues in skin rash Basal cell carcinoma photos is the presence of a fine, raised, and often pearly border that surrounds the erythematous (red) patch. This border may be thin and thread-like, but its translucency and slight elevation are key indicators that distinguish it from the generally uniform borders of inflammatory rashes. Unlike eczema, which often presents with ill-defined margins that blend into the surrounding skin, superficial BCC tends to have a more distinct, though sometimes subtle, boundary. The pearly sheen of this border, even if faint, is a consistent sign of Basal cell carcinoma often highlighted in magnified views within comprehensive Basal cell carcinoma of the skin symptoms pictures collections.
Another distinguishing feature observable in skin rash Basal cell carcinoma images is the chronic and non-responsive nature of the lesion. While common rashes often wax and wane or respond to topical corticosteroids, superficial BCCs will persist for months or even years, slowly enlarging and showing no significant improvement with standard dermatological treatments for inflammation. This persistence is a critical red flag. The redness may fluctuate, and the scaling can vary, but the underlying lesion continues its slow expansion. Patients often report trying various creams without success, a narrative frequently associated with delayed diagnosis of this type of Basal cell carcinoma.
The central area of a superficial Basal cell carcinoma can also exhibit unique visual signs in skin rash images. It may appear slightly atrophic (thinned), scarred, or show areas of regression, while the active tumor cells continue to spread at the periphery. This phenomenon, known as “central clearing,” can further contribute to confusion with ringworm, which also exhibits central clearing. However, in Basal cell carcinoma of the skin symptoms pictures, the advancing border typically maintains its pearly, raised quality, a feature generally absent in fungal infections. Occasionally, superficial BCCs may also exhibit subtle erosions or crusting within the patch, leading to minimal bleeding upon scratching, another sign that sets it apart from typical rashes.
The location of these “rash-like” Basal cell carcinoma lesions is also an important factor. While they can occur anywhere, superficial BCCs are frequently found on the trunk (chest, back), shoulders, and extremities, areas often exposed to intermittent sun but not always as intensely as the face. Skin rash Basal cell carcinoma images often showcase lesions in these locations, reinforcing the association with sun damage. The presence of a persistent, slowly growing, red, scaly patch on the trunk that does not resolve with standard topical therapy should always raise suspicion for superficial Basal cell carcinoma, especially when visual cues like a pearly border are discernible.
Differential diagnosis for skin rash Basal cell carcinoma, when relying on images, often includes:
- Eczema (Dermatitis): Typically itchy, with less defined borders, often bilateral or symmetrical, and responsive to moisturizers and steroids. BCC often has a distinct, raised border.
- Psoriasis: Characterized by well-demarcated, silvery scales on red plaques, often on extensor surfaces (elbows, knees). BCC usually lacks prominent silvery scaling and is often solitary.
- Tinea Corporis (Ringworm): Fungal infection with an annular (ring-shaped) appearance, central clearing, and an active, often vesicular or pustular border. BCC’s border is usually pearly, not vesicular, and fungal tests are negative.
- Actinic Keratosis (AK): Precancerous lesions that are rough, scaly patches on sun-damaged skin. AKs are generally smaller and thinner than superficial BCC, lack the raised, pearly border, and may feel sandpapery.
- Bowen’s Disease (Squamous Cell Carcinoma in situ): Presents as a persistent, red, scaly patch, similar to superficial BCC. It can be visually indistinguishable and often requires biopsy for definitive diagnosis. However, Bowen’s disease often has a more uniform red color and lacks the pearly border of BCC.
The subtle yet persistent nature of superficial Basal cell carcinoma, coupled with its ability to mimic common rashes, makes comprehensive visual guides crucial. Skin rash Basal cell carcinoma of the skin images are invaluable tools for patient education and clinical training, enabling a more informed assessment of persistent erythematous and scaly lesions that deviate from typical inflammatory patterns and potentially harbor underlying malignancy. Emphasizing the subtle pearliness and persistent nature in such images can significantly improve early detection rates for this challenging BCC variant.
Basal cell carcinoma of the skin Treatment
While this article primarily focuses on Basal cell carcinoma of the skin symptoms pictures and visual signs, understanding the range of effective treatments is crucial for patients after a diagnosis. The choice of Basal cell carcinoma treatment depends on several factors, including the type, size, location, and depth of the Basal cell carcinoma, as well as the patient’s overall health and preferences. The primary goal of treatment is always complete removal of the cancer while preserving as much healthy tissue as possible and minimizing scarring, a critical consideration especially for visible lesions on the face highlighted in Basal cell carcinoma of the skin symptoms pictures. Advances in dermatologic surgery and non-surgical options offer diverse approaches to effectively manage Basal cell carcinoma, ensuring high cure rates.
One of the most common and highly effective Basal cell carcinoma treatments is Surgical Excision. This procedure involves cutting out the cancerous tumor along with a surrounding margin of healthy skin (known as the surgical margin). The excised tissue is then sent to a pathology lab to confirm that all cancer cells have been removed, ensuring “clear margins.” Surgical excision is suitable for most types of Basal cell carcinoma, especially smaller, well-defined lesions. Its effectiveness is very high, with cure rates typically above 95%. This method is frequently depicted in medical texts and educational materials as a standard approach, offering a balance of efficacy and cosmetic outcome, particularly for lesions that are not overly large or complex, a common scenario following early detection guided by Basal cell carcinoma of the skin symptoms pictures.
For more complex or high-risk Basal cell carcinoma lesions, especially those on the face, ears, or other cosmetically sensitive areas, Mohs Micrographic Surgery (MMS) is often considered the gold standard. Mohs surgery involves removing the tumor layer by layer, with each layer examined immediately under a microscope. This precise technique allows the surgeon to remove all cancerous cells while preserving the maximum amount of healthy tissue. This meticulous approach results in the highest cure rates for Basal cell carcinoma (up to 99%) and is particularly beneficial for large, recurrent, aggressive, or ill-defined tumors, such as morpheafrom BCC, which are often challenging to fully delineate from Basal cell carcinoma of the skin symptoms pictures alone. The ability to confirm clear margins during the surgery itself minimizes the need for additional procedures and optimizes cosmetic results, a crucial aspect when addressing visible Basal cell carcinoma lesions.
Another widely used Basal cell carcinoma treatment, particularly for superficial lesions often resembling a rash in skin rash Basal cell carcinoma images, is Curettage and Electrodesiccation (ED&C). This procedure involves scraping away the cancerous tissue with a spoon-shaped instrument called a curette, followed by electrocautery (burning) to destroy any remaining cancer cells and control bleeding. This process is typically repeated several times to ensure thorough removal. ED&C is a quick, relatively simple procedure with good cure rates for small, superficial, or nodular Basal cell carcinoma, especially on the trunk and extremities. It generally leaves a small, round, flat scar. While effective, it’s not typically recommended for aggressive subtypes or lesions in high-risk areas due to its reliance on the surgeon’s tactile sense rather than microscopic margin control.
For certain types of Basal cell carcinoma, especially superficial BCCs, Topical Therapies can be a viable non-surgical treatment option. These include:
- Imiquimod Cream (Aldara, Zyclara): An immune response modifier that stimulates the body’s immune system to attack cancer cells. It is applied to the lesion for several weeks and is primarily used for superficial Basal cell carcinoma. The visual resolution of the lesion over time, from its initial appearance in skin rash Basal cell carcinoma images to post-treatment, can be quite dramatic.
- 5-Fluorouracil (5-FU) Cream (Efudex, Carac): A chemotherapeutic agent that selectively kills rapidly dividing cells. Similar to imiquimod, it’s applied topically over several weeks, mainly for superficial Basal cell carcinoma. Patients experience significant inflammation and crusting during treatment, which then subsides.
These topical treatments avoid surgery but require patient compliance and can cause significant local skin reactions (redness, scabbing, discomfort) during the treatment period. Their cure rates are generally lower than surgical methods but are a good option for widespread superficial Basal cell carcinoma or for patients who cannot undergo surgery, offering a non-invasive alternative to address the visually identified Basal cell carcinoma symptoms.
Radiation Therapy is another non-surgical treatment option for Basal cell carcinoma, particularly for patients who are not candidates for surgery due to age, poor health, or the location/size of the tumor (e.g., lesions on the eyelids or nose that would result in significant cosmetic or functional deficits if surgically removed). It involves using high-energy X-rays to destroy cancer cells. Radiation therapy is typically administered in multiple sessions over several weeks. While effective, it can cause skin redness, irritation, and long-term changes in skin texture and color in the treated area. It’s often chosen for recurrent Basal cell carcinoma or when complete surgical removal is challenging, providing an alternative approach to managing various Basal cell carcinoma presentations seen in Basal cell carcinoma of the skin symptoms pictures.
Finally, Cryosurgery (freezing the tumor with liquid nitrogen) can be used for very small, superficial Basal cell carcinoma lesions, especially in patients where a quick, in-office procedure is desired. The freezing causes the cancer cells to die, and the treated area forms a blister and then a scab, which eventually falls off. While convenient, its cure rates are generally lower than surgical methods, and it’s not suitable for larger, deeper, or aggressive Basal cell carcinoma types due to the lack of margin control. Similarly, Photodynamic Therapy (PDT), which involves applying a photosensitizing agent to the skin and then activating it with a specific light source, can be used for superficial Basal cell carcinoma. This treatment induces cell death in cancerous tissue, offering another non-invasive route. These diverse Basal cell carcinoma treatment modalities underscore the importance of accurate diagnosis, often guided by detailed Basal cell carcinoma of the skin symptoms pictures, to select the most appropriate and effective therapy for each individual case, aiming for optimal outcomes in terms of cancer clearance and cosmetic appearance.