
Understanding is crucial for prompt recognition and medical intervention. This article meticulously details the visual presentation of Erysipelas, from its initial subtle manifestations to its full-blown, characteristic appearance, providing a comprehensive guide to identifying this bacterial skin infection.
Erysipelas Symptoms Pictures
Erysipelas presents a distinctive and often dramatic visual picture on the skin, making its highly recognizable once familiarized. The affected area typically appears as a bright, fiery red patch that is sharply demarcated from the surrounding healthy skin. This clear border, often palpable as a raised edge, is one of the hallmark . The color can range from a vivid scarlet to a deeper crimson, sometimes with a purplish hue in more severe or chronic cases, or in individuals with darker skin tones where erythema can be less obvious.
The skin within the infected region is typically swollen, tense, and feels noticeably warm or hot to the touch. This induration is a key feature, contributing to the glossy, stretched appearance of the skin, which can sometimes resemble an orange peel texture, known as “peau d’orange,” especially when lymphatic drainage is significantly impaired. This particular texture is a strong indicator of underlying inflammation and fluid accumulation, making it a critical aspect when examining .
Further visual characteristics include the potential for blistering (vesicles) or larger fluid-filled sacs (bullae) to form on the surface of the erythematous patch. These indicate a more severe inflammatory response and can sometimes rupture, leading to weeping or crusting. In rare, severe instances, hemorrhagic bullae or even necrotic areas (tissue death) can develop, appearing as dark, purplish-black patches, signifying a critical progression of the disease and requiring immediate attention as these are advanced .
Common locations for Erysipelas are the face, particularly around the nose and cheeks, often presenting in a “butterfly” distribution, and the lower limbs, especially the legs and feet. will often show pronounced swelling around the eyes and cheeks, sometimes making it difficult for the patient to open their eyes fully. On the other hand, frequently depict the infection spreading rapidly up the calf or shin, highlighting the characteristic raised border and fiery redness.
Associated symptoms that manifest alongside these visual changes contribute to the patient’s overall distress and aid in diagnosis. These include:
- The affected area is usually very tender and painful to touch, and even light contact can cause significant discomfort, contributing to the patient’s reluctance to move or have the area examined.
- Patients often describe a sensation of intense burning or heat emanating from the infected skin, consistent with the objective warmth observed.
- Fever and chills are extremely common and can precede the visible skin rash. The onset of these constitutional symptoms is often abrupt and severe, indicating a systemic response to the bacterial infection.
- A general feeling of unwellness, body aches, and profound fatigue frequently accompany the infection, reflecting the body’s battle against the spreading bacteria.
- Red streaks extending from the main lesion, following the lymphatic pathways, can sometimes be seen. These indicate inflammation of the lymphatic vessels and signal the spread of the infection towards regional lymph nodes.
- Swollen and tender lymph nodes in the area draining the infected site (e.g., cervical nodes for facial Erysipelas, inguinal nodes for leg Erysipelas) are common, further underscoring the systemic nature of the infection and offering additional diagnostic clues to .
The rapid progression of these , from a small patch to a widespread area within hours to a day, is another critical characteristic that helps differentiate it from other less aggressive skin conditions. Close observation of the evolving lesion in can therefore be highly informative for healthcare providers. Understanding these detailed visual and associated symptoms is key for anyone trying to identify in its typical presentation.

Signs of Erysipelas Pictures
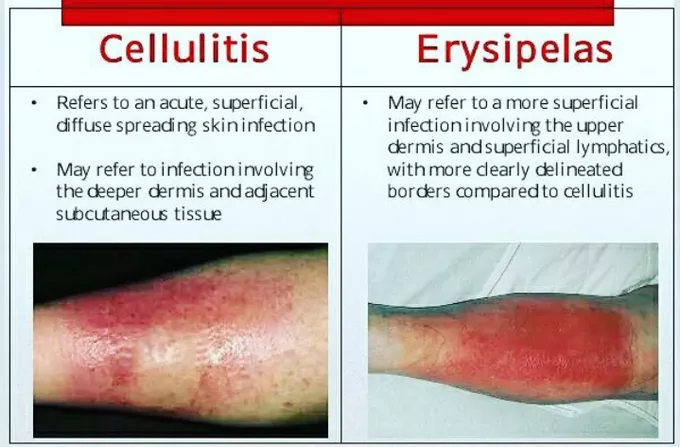
Identifying the distinct involves focusing on specific visual markers that differentiate it from other dermatological conditions, such as cellulitis or contact dermatitis. While Erysipelas and cellulitis are both bacterial skin infections, the visual presentation offers key distinctions critical for accurate diagnosis and effective treatment. The defining characteristic of Erysipelas, vividly captured in , is its notably raised and sharply demarcated border.
This raised margin is not merely a subtle difference; it is often palpable, giving the infected area a cliff-like edge separating it from the unaffected skin. This feature is particularly evident in . In contrast, cellulitis typically presents with a more diffuse, ill-defined border that blends gradually into the surrounding skin, making it harder to pinpoint the exact perimeter of the infection. This sharp contrast is one of the most reliable .
The texture of the affected skin in Erysipelas is another significant sign. It usually appears tense, glossy, and sometimes almost “stretched” due to underlying edema and inflammation. This turgidity can be so pronounced that the skin takes on the aforementioned “peau d’orange” appearance, a pattern of pitting resembling an orange peel, especially visible on the lower limbs and face. are therefore crucial for understanding this specific visual sign indicating significant lymphatic involvement.
Beyond the primary erythema and swelling, several other warrant close inspection:
- The presence of small fluid-filled blisters (vesicles) or larger bullae (blisters greater than 0.5 cm) on the surface of the erythematous skin indicates a more intense inflammatory response. These suggest deeper involvement and potential for epidermal detachment.
- In some cases, small petechiae (pinpoint hemorrhages) or purpura (larger purple spots) may develop within the erythematous patch. These signal capillary damage and can be a sign of more severe infection, sometimes preceding necrosis.
- Though less common, severe Erysipelas can lead to tissue necrosis, where parts of the skin turn dark purplish-black and eventually slough off, forming ulcers. These represent a critical and severe complication requiring urgent medical intervention.
- The appearance of red lines or streaks extending proximally from the main Erysipelas lesion is a strong indicator of lymphatic spread. These visually demonstrate the infection’s progression along the lymphatic channels, often towards regional lymph nodes.
- Palpably enlarged and tender lymph nodes in the drainage area of the infection are a common systemic sign. While not a direct skin sign, their presence strongly corroborates the diagnosis of Erysipelas and indicates the body’s immune response to the spreading bacteria, frequently seen in .
- The dynamic nature of Erysipelas is a key diagnostic sign. The lesion often expands rapidly, sometimes visibly growing within a matter of hours. Documenting this through sequential imaging can provide strong evidence for the diagnosis.
The localization of Erysipelas also provides important diagnostic clues. frequently involve the bridge of the nose, cheeks, and periorbital areas, often forming a characteristic “butterfly” distribution. This central facial involvement is less common in typical cellulitis. For , the infection commonly affects the lower leg, often originating from a breach in the skin like tinea pedis or a minor wound. Observing these specific presentations in enhances diagnostic accuracy.
Furthermore, the systemic symptoms that often precede or accompany the skin signs – such as sudden onset of high fever, chills, malaise, and headache – are crucial in the overall assessment. These constitutional symptoms, when seen in conjunction with the characteristic skin lesions, paint a clear picture of an acute bacterial infection. Recognizing these combined from both the visual perspective and patient history is paramount for timely and effective management, directly influencing the accuracy of .
Early Erysipelas Photos
Recognizing is essential for prompt treatment and preventing widespread infection and potential complications. Unlike the dramatic presentation of fully developed Erysipelas, the initial stages can be subtle, sometimes leading to misdiagnosis or delayed care. The onset of Erysipelas is typically acute, with symptoms often appearing within hours or a day of a precipitating event or skin breach.
The often manifest as a small, slightly raised, tender, and warm patch of redness on the skin. This initial lesion might not yet exhibit the sharp demarcation characteristic of later stages, making it crucial to look for other subtle cues. Patients might first notice a feeling of warmth, tightness, or a mild burning sensation in a localized area, which then progresses to visible redness. can be challenging to distinguish from common irritations or insect bites at this very early phase.
Key indicators to look for in include:
- The first visible sign is usually a patch of redness that might be faint at first but quickly intensifies. This erythema often has a somewhat irregular but developing border, indicating the initial spread of the bacteria.
- Even before pronounced redness, the area often feels abnormally warm to the touch and is sensitive or tender to palpation. This localized heat is a direct result of the inflammatory process initiated by the bacterial invasion.
- A subtle puffiness or firmness of the skin may be present, indicating early edema. This initial swelling contributes to the slightly raised feel of the lesion, which will become more prominent as the infection progresses.
- One of the most telling signs of is the speed at which the lesion expands. An initial small patch of redness can grow significantly in size over a few hours, becoming more vivid in color and more defined in its border. Sequential taken hours apart can starkly illustrate this rapid expansion.
- While not directly visible on the skin, systemic symptoms often precede the rash by several hours. Patients might experience a sudden onset of high fever (often 102-104°F or 39-40°C), chills, malaise, headache, and even nausea or vomiting. These are critical clues that a significant infection is brewing, even if the skin changes are still subtle.
- Often, there is an identifiable minor break in the skin at or near the site of onset. This could be a small cut, an insect bite, a scratch, an area of tinea pedis (athlete’s foot), or even a surgical incision. While not always obvious in , the patient’s history can pinpoint this initial portal for bacterial entry.
For example, might show a small, slightly red and swollen area near the nose or mouth, which quickly expands to encompass a larger portion of the cheek. Similarly, might start as a patch of redness around an insect bite or a scratch on the lower leg, becoming increasingly distinct and fiery over a short period. The border, while not yet the sharply demarcated “cliff edge,” begins to solidify and become more pronounced as the infection progresses beyond its initial hours.
The differential diagnosis in these early stages can be broad, including contact dermatitis, insect bites, or even a localized allergic reaction. However, the presence of accompanying high fever, chills, and the rapid, progressive nature of the skin changes are strong indicators pointing towards Erysipelas. Careful attention to these , combined with a thorough patient history regarding the sudden onset of systemic illness, empowers healthcare providers to make an early and accurate diagnosis, significantly improving patient outcomes by allowing timely antibiotic therapy before the infection becomes more entrenched and visually dramatic, as depicted in later-stage .
Skin rash Erysipelas Images
The are characterized by a highly distinctive appearance that sets it apart from many other dermatological conditions. The rash is not merely red; it possesses a fiery, intense erythema that often appears polished or glazed due to the significant underlying edema and inflammation. This specific type of redness, combined with its raised and sharply demarcated border, forms the classic visual signature of Erysipelas, prominently featured in .
Delving deeper into the characteristics of the , we observe several key features:
- The color of the Erysipelas rash typically ranges from bright scarlet to deep crimson. In more severe cases or individuals with darker skin tones, it can appear purplish or violaceous. The intensity of the color usually correlates with the severity of the inflammatory process, making a common search term for visual diagnosis.
- The affected skin feels tense and firm to the touch, reflecting significant swelling (edema). This turgidity contributes to a glossy, stretched appearance. In areas where lymphatic drainage is compromised, the “peau d’orange” texture, characterized by prominent hair follicles giving an orange peel-like dimpling, becomes particularly evident. This is a very specific visual sign in .
- The most consistent and defining characteristic of the Erysipelas rash is its raised, well-demarcated border, often described as a “cliff-like” edge. This distinct separation from healthy skin is crucial for differentiating Erysipelas from cellulitis, which typically has a more diffuse and ill-defined margin. highlight this critical feature.
- As the inflammation intensifies, small blisters (vesicles) or larger fluid-filled bullae may form on the surface of the erythematous rash. These indicate a more severe epidermal involvement and can lead to crusting and weeping if they rupture.
- In some severe instances, the rash may exhibit petechiae (small, pinpoint red or purple spots) or purpura (larger discolored areas) due to capillary leakage. These signify vascular damage and can sometimes precede areas of necrosis, appearing as darker, almost bruised-looking patches.
- Often affects the central face, particularly the nose, cheeks, and periorbital region. It frequently presents in a “butterfly” pattern, crossing the bridge of the nose, making quite recognizable. Swelling around the eyes can be so severe as to impede vision.
- Commonly involves the lower limbs, especially the calf or shin. The rash spreads rapidly upwards, often from a minor skin break on the foot or ankle. typically show a wide area of fiery redness with the characteristic raised border, often accompanied by significant limb swelling.
- Red streaking (lymphangitis) extending from the main rash area, following the lymphatic vessels, is another important visual sign. This indicates the spread of bacteria through the lymphatic system and is frequently observed in .
- As the Erysipelas rash heals, the affected skin may peel or flake off (desquamation), similar to a severe sunburn. This post-inflammatory change is a common sight in , indicating the resolution of the acute infection but sometimes leaving behind temporary hyperpigmentation.
- Repeated episodes of Erysipelas in the same area can lead to chronic changes, such as persistent lymphedema (swelling due to lymphatic damage), thickening of the skin (fibrosis), and altered skin texture. These show a less acute presentation, with more induration and less vivid erythema, but often with chronic swelling.
Understanding the full spectrum of these is vital for healthcare professionals and patients alike. The ability to distinguish the specific visual nuances of the Erysipelas rash, from its distinct border and intense color to its potential for blistering and specific anatomical patterns, significantly aids in early and accurate diagnosis. These detailed visual descriptions, supported by , underscore the importance of visual examination in managing this acute bacterial skin infection effectively.
Erysipelas Treatment
While this article primarily focuses on and visual identification, understanding the regimen is crucial because prompt and effective therapy directly influences the resolution of these visible symptoms and prevents complications. The core of Erysipelas treatment involves antibiotics, which target the bacterial infection, predominantly . The choice and route of administration of antibiotics depend on the severity of the infection and the patient’s overall health.
Antibiotic Therapy: The Cornerstone of Erysipelas Treatment
The primary goal of antibiotic treatment is to eradicate the causative bacteria, thereby stopping the progression of the visible skin rash and systemic symptoms. The selection of antibiotics is usually guided by the suspected pathogen and local resistance patterns.
- Penicillin remains the first-line treatment for Erysipelas due to its effectiveness against .
- Often prescribed for milder cases of Erysipelas, where the patient is not systemically ill and can tolerate oral medication. typically involves a 7-14 day course. Visual improvement, such as fading redness and reduced swelling, should be observed within 24-48 hours.
- Recommended for more severe infections, especially when patients exhibit significant systemic symptoms (high fever, chills, profound malaise), extensive skin involvement, rapid progression, or an inability to tolerate oral medications. ensures rapid attainment of therapeutic drug levels, which can quickly halt the visible spread of the rash and bring down fever. Hospitalization is usually required for IV administration, and patients are typically switched to oral antibiotics once significant clinical improvement in is observed.
- For patients with penicillin allergies, or in cases where methicillin-resistant (MRSA) is suspected (though less common for classic Erysipelas), alternative antibiotics are used.
- Suitable alternatives for penicillin-allergic individuals. These macrolides and lincosamides are effective against streptococcal infections.
- Another option, often used, but should be avoided in patients with severe penicillin allergies due to potential cross-reactivity.
- May be considered in specific circumstances, especially if MRSA co-infection is a concern, though these are not typical first-line for uncomplicated Erysipelas.
Supportive Care Measures: Alleviating Symptoms and Aiding Recovery
In addition to antibiotics, supportive care plays a vital role in managing discomfort, promoting healing, and preventing complications, directly influencing how the .
- Elevating the infected limb (e.g., resting an infected leg on pillows) helps reduce swelling and discomfort by promoting lymphatic and venous drainage. This directly contributes to the reduction in the tense, glossy appearance of the skin seen in .
- Applying cool, moist compresses to the affected area can help relieve the burning sensation and reduce inflammation. Care should be taken to ensure the compresses are clean and not excessively cold, which could impede circulation.
- Over-the-counter pain relievers such as paracetamol (acetaminophen) or ibuprofen can help manage pain, fever, and discomfort associated with the infection.
- Keeping the skin clean and dry, especially if blistering or weeping is present, is crucial. Avoidance of harsh soaps or irritants can prevent further skin breakdown and facilitate healing of the .
- Maintaining adequate fluid intake is important, especially when fever is present, to prevent dehydration and support overall recovery.
Addressing Predisposing Factors: Preventing Recurrence
Erysipelas often recurs, particularly in individuals with underlying conditions that impair skin integrity or lymphatic drainage. Addressing these is a critical part of a comprehensive treatment plan to prevent future episodes and improve the long-term prognosis of the .
- Fungal infections between the toes can create breaches in the skin, serving as entry points for bacteria. Aggressive treatment of athlete’s foot with antifungal creams or oral medications is essential, as even minor cracks can initiate a new Erysipelas infection, visually observed as recurrent .
- Chronic swelling, often due to impaired lymphatic drainage (e.g., after surgery, radiation, or venous insufficiency), significantly increases the risk of Erysipelas. Compression garments, manual lymphatic drainage, and vigilant skin care are vital in managing lymphedema and reducing skin susceptibility to infection, thus altering the visual presentation of chronic .
- Conditions that cause poor circulation and chronic leg swelling can also predispose to Erysipelas. Managing these conditions with compression stockings and leg elevation is crucial.
- Any break in the skin barrier, from minor cuts to insect bites or surgical incisions, can be a portal of entry. Proper wound care and prompt treatment of any skin injury are important preventative measures.
- For individuals with frequent, recurrent episodes of Erysipelas (e.g., 2 or more episodes per year), low-dose, long-term prophylactic antibiotics (e.g., penicillin V) may be prescribed to prevent recurrence. This preventative measure directly reduces the likelihood of future and the associated visual skin changes.
Monitoring Treatment Response: Visual Cues of Healing
The effectiveness of is monitored by observing both systemic and local symptoms. Visually, improvement should be evident within 24-48 hours of starting appropriate antibiotics:
- The fiery red color of the rash should begin to subside, becoming less intense and eventually fading to a pinkish hue.
- The tense, swollen appearance of the skin should diminish, and the area should feel softer to the touch.
- While the sharp demarcation may persist for a while, the raised “cliff edge” should become less prominent.
- The subjective symptoms of pain, tenderness, and warmth should significantly decrease.
- If present, blisters should dry up and begin to resolve.
Failure to observe these improvements in after 48-72 hours of treatment warrants re-evaluation of the diagnosis, the antibiotic choice, or consideration of potential complications like abscess formation. Overall, a clear understanding of and its impact on the visible symptoms is integral to effective patient care, from initial diagnosis guided by to full recovery and prevention of recurrence.