This detailed guide provides an in-depth look into Xanthelasma symptoms pictures, offering comprehensive descriptions of how these cholesterol deposits present visually on the eyelids and surrounding areas. Understanding the specific visual characteristics is crucial for accurate identification.
Xanthelasma Symptoms Pictures
This section meticulously details the visual presentation and characteristics that would be apparent in Xanthelasma symptoms pictures, aiding in the recognition of these distinct lesions. Xanthelasma palpebrarum, often referred to simply as Xanthelasma, manifests as specific dermal deposits primarily around the eyelids. Recognizing these visual cues is fundamental for differentiating Xanthelasma from other skin conditions affecting the periorbital region. The appearance is quite characteristic, making visual identification a key diagnostic step for these eyelid cholesterol deposits.
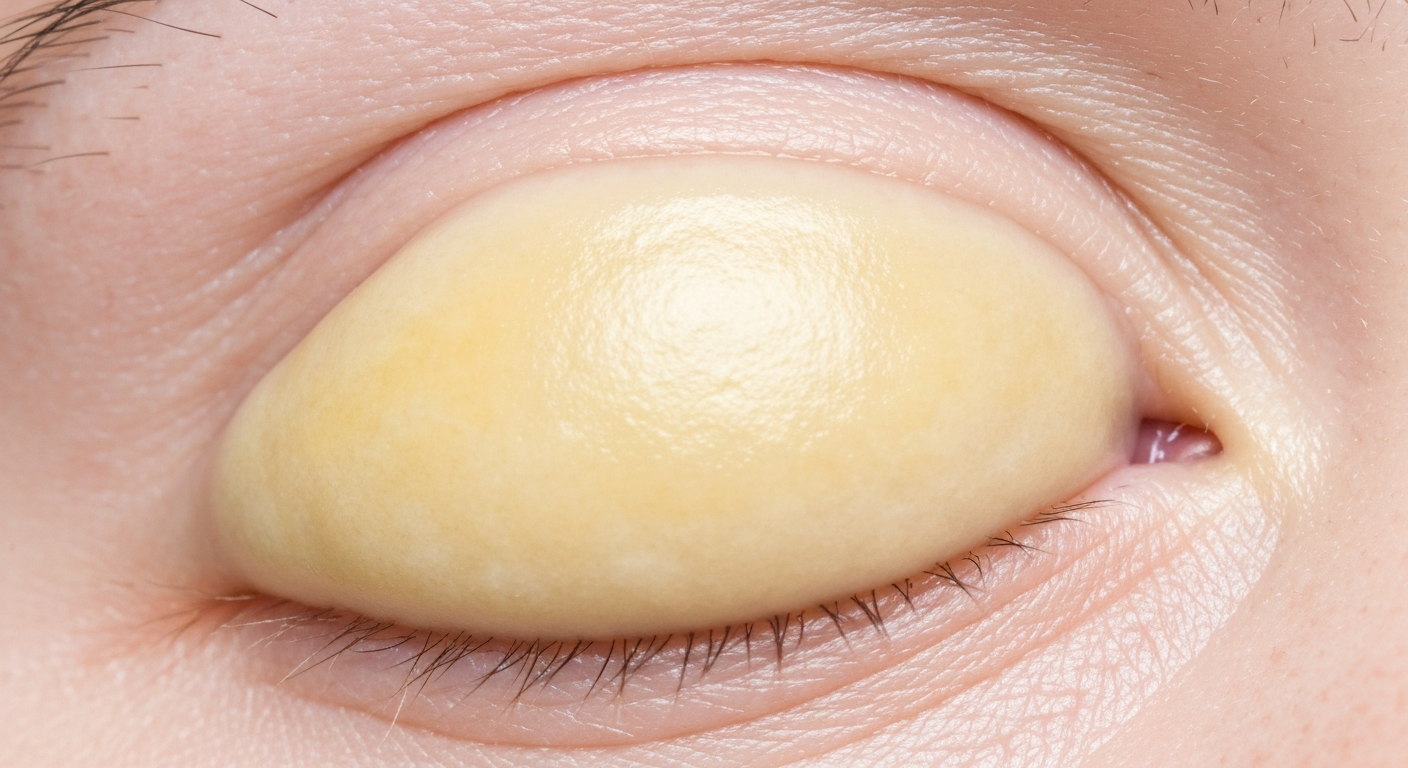
The primary visual symptom is the presence of yellow or yellowish-white plaques. These plaques are typically:
- Coloration: Predominantly a dull yellow to an ochre or creamy white hue. The intensity of the yellow can vary, sometimes appearing paler, almost off-white, and at other times displaying a more saturated, buttery yellow. This discoloration, clearly visible in Xanthelasma symptoms pictures, is due to the accumulation of lipid-laden macrophages, also known as foam cells, within the dermis. This fatty deposit in the skin gives it its characteristic appearance.
- Location: Most commonly observed on the eyelids. The inner canthus (the corner of the eye closest to the nose) is a particularly frequent site for these periorbital lesions, but plaques can extend across the entire eyelid, affecting both the upper and lower lids. They can also appear in the medial or lateral aspects of the eyelids, sometimes forming a semi-circular or irregular band. These ocular region lipid deposits are highly specific in their localization.
- Shape and Borders: Often appear as flat or slightly raised lesions. Their borders can be well-defined and distinct, or they can gradually blend into the surrounding normal skin, especially in early or diffuse presentations. Shapes vary from small, discrete spots to larger, irregular patches. Some plaques might have a somewhat lobulated or segmented appearance, which would be evident in high-resolution Xanthelasma symptoms pictures.
- Texture: The surface of Xanthelasma plaques is typically smooth and soft to the touch. They are non-tender and non-pruritic, meaning they usually do not cause pain or itching, which distinguishes them from many inflammatory skin rashes. The skin overlying the plaques retains its normal elasticity in most cases, though larger lesions might slightly stretch or distend the eyelid skin. This smooth texture is a consistent feature in Xanthelasma.
- Size: Can range from a few millimeters in diameter to several centimeters. They often begin as small, pinpoint yellowish spots that gradually enlarge and coalesce over time, forming larger, more conspicuous plaques. The growth rate is usually slow and progressive, a key aspect to observe when comparing sequential Xanthelasma symptoms pictures.
- Symmetry: While Xanthelasma can affect only one eye (unilateral), it frequently presents bilaterally, appearing on both eyelids, often in a somewhat symmetrical fashion. However, the size and exact location might differ slightly between the two eyes, a point for careful observation in any set of Xanthelasma symptoms pictures.
- Number of Lesions: Patients may present with a single plaque, but it is common to observe multiple lesions on one or both eyelids. These multiple lesions can remain discrete or merge into larger, confluent areas, contributing to a more extensive visual presentation of the condition.
- Consistency: When palpated gently, Xanthelasma lesions typically feel soft or slightly doughy. They are not hard or indurated like some other skin growths or cancerous lesions. This soft consistency is a key physical finding that would be indirectly suggested by clear Xanthelasma symptoms pictures showing their subtle elevation and smooth texture.
- Associated Features: Xanthelasma itself is a benign skin condition. However, its presence often serves as a visual indicator of underlying dyslipidemia, particularly elevated low-density lipoprotein (LDL) cholesterol or triglycerides. While the plaques themselves are a symptom of local lipid deposition, their appearance should prompt further investigation into the patient’s lipid profile. This link to systemic cholesterol levels makes the visual symptom particularly significant.
Understanding these detailed visual characteristics is paramount for anyone studying Xanthelasma symptoms pictures, ensuring accurate identification and appropriate clinical management. The non-inflammatory nature and distinct yellow coloration make these lesions quite unique in their presentation on the delicate eyelid skin, distinguishing them from other types of eyelid lesions.
Signs of Xanthelasma Pictures
Observing signs of Xanthelasma pictures allows for a deeper understanding of the clinical indicators that differentiate this condition. While symptoms refer to what the patient experiences, signs are objective findings identified by an observer or clinician. For Xanthelasma, these signs are almost entirely visual. The periorbital location is a cardinal sign, with lipid deposition occurring specifically in the superficial dermis of the eyelids. These characteristic lipid deposits are a visible manifestation of intracellular cholesterol accumulation, often linked to elevated cholesterol levels. The specific eyelid skin changes are crucial for diagnosis.
Key observable signs that would be prominent in diagnostic signs of Xanthelasma pictures include:
- Topographical Distribution: The preference for the medial canthus is a strong diagnostic sign. Plaques often initiate near the nasal side of the upper eyelid and can spread laterally or inferiorly. Lower eyelid involvement is also common, frequently mirroring the pattern on the upper lid. The precise anatomical locations that often show these periorbital xanthomas include:
- Medial aspect of the upper eyelid, close to the nose, forming characteristic yellow lesions.
- Medial aspect of the lower eyelid, often slightly below the tear duct.
- Central upper eyelid, sometimes extending towards the eyebrow.
- Central lower eyelid, occasionally forming a band just below the lash line.
- Lateral aspects of both upper and lower eyelids, though less common as primary sites for Xanthelasma signs.
- Morphological Progression: Clinicians often observe a slow but steady growth pattern. What starts as a small macule (flat spot) or papule (raised bump) can gradually expand and become more plaque-like. This progression is evident over months to years, and subsequent signs of Xanthelasma pictures taken at different times can illustrate this enlargement of the fatty deposits. The lesions do not typically regress spontaneously.
- Non-Inflammatory Nature: A critical sign distinguishing Xanthelasma from various dermatological conditions is the complete absence of inflammation. There is no redness (erythema), heat, swelling (edema), or pain associated with these lesions. The surrounding skin remains normal in appearance, without signs of irritation or infection. This non-inflammatory characteristic is consistently visible in high-quality Xanthelasma imagery, setting it apart from inflammatory conditions.
- Homogeneous Appearance: While the size and shape may vary, the internal texture and color within a single Xanthelasma plaque are usually homogeneous. There are no variegated colors, ulcerations, crusting, or bleeding, which are often indicative of other skin pathologies. The surface remains intact and smooth, a consistent sign of lipid deposition.
- Response to Palpation: Gentle palpation reveals a soft or slightly rubbery consistency. The lesions are movable with the underlying skin and are not fixed to deeper structures. This tactile sign complements the visual assessment of Xanthelasma, providing additional diagnostic information.
- Associated Systemic Lipid Disorders: Although not a direct visual sign on the skin itself, the presence of Xanthelasma is a strong clinical indicator that often prompts investigation for underlying dyslipidemia. Roughly 50% of individuals with Xanthelasma have elevated serum cholesterol or triglyceride levels. This association is a crucial diagnostic sign, directing further medical evaluation. Conditions often linked to these eyelid plaques include:
- Hypercholesterolemia (elevated total cholesterol), a common underlying cause of Xanthelasma.
- Hypertriglyceridemia (elevated triglycerides).
- Familial hypercholesterolemia (genetic lipid disorder).
- Primary biliary cholangitis (a liver disease).
- Hypothyroidism (underactive thyroid).
- Diabetes mellitus.
- Nephrotic syndrome (kidney disorder).
- Distinction from Other Xanthomas: It is important to note that Xanthelasma is a specific type of xanthoma, which refers to localized collections of lipid-laden macrophages. However, Xanthelasma is specifically limited to the eyelids. Other types of xanthomas (e.g., eruptive, tuberous, tendinous, planar) occur at different body sites and have distinct morphologies, making the periorbital location a definitive diagnostic sign in signs of Xanthelasma pictures.
Careful examination of these objective signs, particularly as depicted in clinical photographs, is essential for a precise diagnosis of Xanthelasma. The characteristic appearance and location leave little ambiguity when compared to other eyelid pathologies, confirming the presence of these distinctive lipid plaques.
Early Xanthelasma Photos
Examining early Xanthelasma photos provides invaluable insight into the initial stages of this skin condition, showing how these lipid deposits first begin to manifest before they become more prominent. Recognizing these subtle initial changes can be challenging but is crucial for early detection, which can inform discussions about underlying health and potential treatment options for nascent plaques. Early lesions are typically less conspicuous and might be overlooked without careful examination.
The progression of Xanthelasma often follows a pattern, which can be visually tracked through serial early Xanthelasma photos:
- Initial Appearance as Small Macules: Xanthelasma often begins as very small, flat, yellowish discolorations. These macules may be only 1-2 millimeters in diameter, easily mistaken for a slight variation in skin tone or a natural skin crease, especially in individuals with lighter skin tones. The yellow hue might be faint, almost translucent, making them difficult to spot without close inspection. This initial presentation of subtle yellowing is a key indicator.
- Subtle Elevation: As the lipid deposits accumulate, these macules can transform into slightly raised papules. This elevation is usually minimal in the early stages, feeling more like a subtle thickening of the skin rather than a distinct bump. The surface remains smooth and non-scaly, differentiating these minor eyelid discolorations from other skin growths.
- Faint Yellowish Tint: In early Xanthelasma photos, the yellow color may not be as vibrant or distinct as in more advanced plaques. It can be a very light, straw-yellow or creamy-white shade, blending subtly with the surrounding skin. This faintness is a hallmark of nascent lesions, indicating lipid accumulation beneath the surface.
- Unilateral or Asymmetrical Onset: While Xanthelasma commonly becomes bilateral, its onset can be unilateral or highly asymmetrical. An early Xanthelasma photo might show a single, small lesion on one eyelid, with the other eyelid appearing completely clear. Over time, similar lesions may develop on the contralateral eyelid, progressing to bilateral involvement.
- Location Predilection (Medial Canthus): Even in its early stages, Xanthelasma frequently favors the medial canthus. An early Xanthelasma photo will often show a small, yellowish speck or streak near the inner corner of the upper eyelid, extending towards the nasal bridge. This specific localization provides a strong clue for early diagnosis of these developing eyelid lesions.
- Slow and Insidious Growth: The development of Xanthelasma is typically very slow and insidious. Lesions do not appear overnight but rather evolve gradually over months to years. This slow progression means that early Xanthelasma photos might only show marginal changes over short periods, necessitating regular monitoring for growth of these early lipid deposits.
- Absence of Symptoms: In the early phases, patients are almost always asymptomatic. There is no itching, pain, burning, or discomfort associated with these small lesions. Their presence is purely cosmetic, or they are discovered incidentally during a routine eye or skin examination, highlighting their silent nature.
- Non-Palpable or Barely Palpable: Very early macules might be non-palpable. As they progress to papules, they become barely palpable, feeling soft and indistinguishable from the surrounding skin texture without careful attention. This makes early detection reliant on visual inspection.
- Lack of Inflammatory Response: Crucially, even early Xanthelasma does not show signs of inflammation. There is no erythema (redness) or warmth around the nascent plaques, distinguishing them from inflammatory skin conditions that might also present as small bumps. This non-inflammatory aspect is consistently seen in early Xanthelasma photos.
Understanding these specific features of early Xanthelasma photos is vital for healthcare professionals and individuals alike. Early detection can prompt investigation into lipid profiles, allowing for earlier management of potential underlying systemic conditions. While cosmetically minor in early stages, the potential systemic implications make early recognition significant. The subtle visual cues, such as faint yellowing and slight elevation, particularly in the medial canthal region, are critical for discerning these developing lesions and for addressing eyelid skin manifestation effectively.
Skin rash Xanthelasma Images
While Xanthelasma is not a “skin rash” in the typical inflammatory sense, the term skin rash Xanthelasma images refers to how these distinct lipid deposits appear on the skin surface, differentiating them from common dermatological eruptions. It is critical to understand that Xanthelasma does not present with the typical features of an acute inflammatory rash, such as redness, itching, vesicles, or scaling. Instead, its appearance is characterized by chronic, non-inflammatory plaques, which are distinct from typical skin rashes.
When viewing skin rash Xanthelasma images, key differentiating features from conventional rashes include:
- Non-Inflammatory Appearance: This is the most significant distinction. A typical “skin rash” often implies inflammation, characterized by:
- Erythema (Redness): Absent in Xanthelasma. The skin surrounding and overlying the plaques retains its normal color.
- Edema (Swelling): Minimal or absent, unlike the puffiness seen in many rashes. The elevation of Xanthelasma is due to tissue deposition, not fluid accumulation.
- Pruritus (Itching) or Pain: Xanthelasma is typically asymptomatic in terms of sensation. Rashes, by contrast, are often itchy, painful, or burning.
- Heat: No increased warmth is associated with Xanthelasma.
In skin rash Xanthelasma images, the lack of these inflammatory signs is consistently observable, highlighting the condition’s benign and non-reactive nature of these non-inflammatory plaques.
- Characteristic Coloration: The yellow or yellowish-white color is a defining feature that sets it apart from the diverse color palette of rashes (red, pink, purple, brown). This specific xanthochromia is due to intracellular lipid accumulation, clearly visible in Xanthelasma skin images.
- Smooth, Intact Surface: Unlike many rashes that present with vesicles, pustules, crusts, scales, or excoriations (scratch marks), Xanthelasma plaques maintain a smooth, often slightly shiny, and intact surface. The skin barrier is preserved, a characteristic of these dermal deposits.
- Fixed Morphology: Rashes can change rapidly in appearance, sometimes within hours or days, exhibiting different stages of evolution (e.g., papules turning into vesicles, then crusts). Xanthelasma, however, has a stable morphology, growing slowly over extended periods without acute changes. Skin rash Xanthelasma images would show this consistent appearance over time, barring treatment, confirming its nature as a specific skin lesion.
- Localized to Eyelids: While some rashes can be localized, Xanthelasma has a very specific predilection for the periorbital area, particularly the eyelids. If a similar lesion were found elsewhere on the body, it would likely be classified as a different type of xanthoma (e.g., planar xanthoma), further distinguishing Xanthelasma as a specific eyelid manifestation.
- Absence of Systemic Acute Symptoms: Rashes can often be accompanied by systemic symptoms like fever, malaise, or lymphadenopathy. Xanthelasma itself does not cause such acute systemic reactions; any systemic symptoms would be related to an underlying condition (like hyperlipidemia), not directly to the skin lesions.
- Comparison to Other Eyelid Conditions: When examining skin rash Xanthelasma images, it’s important to distinguish it from other conditions that might superficially resemble a “rash” on the eyelids:
- Allergic Contact Dermatitis: Characterized by redness, severe itching, swelling, and sometimes blistering or oozing, clearly different from the smooth, yellow Xanthelasma.
- Seborrheic Dermatitis: Presents with greasy, yellowish scales, erythema, and itching, particularly at the lash line. While it can have a yellowish tint, the scales and inflammation differ significantly from Xanthelasma.
- Milia: Small, white or yellowish cysts, but they are typically very small, firm, and contain keratin, not lipids.
- Syringomas: Small, skin-colored or slightly yellowish papules, but they are usually smaller, firmer, and do not coalesce into plaques in the same manner as Xanthelasma.
- Nevi (Moles): Can be pigmented or skin-colored but have distinct cellular characteristics and often a different growth pattern.
Therefore, while the heading refers to “skin rash Xanthelasma images,” it’s crucial to interpret this as a detailed description of Xanthelasma’s visual presentation on the skin, explicitly contrasting it with the inflammatory nature of a typical rash. The non-inflammatory, distinctively yellow, smooth plaques on the eyelids are highly characteristic of this specific eyelid skin manifestation.
Xanthelasma Treatment
Once Xanthelasma symptoms pictures have confirmed the diagnosis, patients often seek effective treatment, primarily for cosmetic reasons. While Xanthelasma is benign and generally asymptomatic, its visible presence on the eyelids can be a source of significant self-consciousness. It’s important to note that treating Xanthelasma cosmetically does not address any underlying lipid disorder; therefore, systemic evaluation and management of dyslipidemia are crucial alongside local treatment. Recurrence is possible, especially if underlying lipid abnormalities are not controlled, necessitating comprehensive Xanthelasma removal strategies.
A variety of methods are employed for Xanthelasma treatment, each with its own advantages and potential considerations:
1. Surgical Excision
This is one of the most common and effective methods for Xanthelasma treatment, particularly for smaller to medium-sized lesions.
- Procedure: The plaques are surgically cut out using a scalpel. Local anesthesia is used. The wound is then closed with fine sutures.
- Advantages: Provides immediate removal of the lesion, offers a high success rate, and allows for histopathological examination of the excised tissue to confirm diagnosis and rule out other conditions. This method offers definitive Xanthelasma removal.
- Considerations: Involves a small scar, which is usually well-hidden in the natural skin folds of the eyelid. There is a risk of ectropion (eversion of the eyelid) or entropion (inversion of the eyelid) if too much skin is removed, especially from the lower eyelid. Recovery involves suture removal and minor swelling/bruising.
- Suitability: Best for discrete, well-defined lesions and when a definitive pathological diagnosis is desired, making it a preferred surgical treatment option.
2. Laser Ablation
Various types of lasers are used in Xanthelasma treatment, targeting the lipid-laden cells, and represent a modern approach to Xanthelasma removal.
- Types of Lasers:
- CO2 Laser: A common choice, it precisely ablates (vaporizes) the Xanthelasma tissue layer by layer. It offers excellent control and minimizes damage to surrounding tissue, making it a popular laser treatment.
- Erbium:YAG Laser: Similar to CO2 but with less thermal damage, leading to faster healing and potentially less scarring, offering a gentle laser removal option.
- Nd:YAG Laser (Q-switched): Sometimes used for smaller or flatter lesions, but less common than ablative lasers for comprehensive Xanthelasma treatment.
- Procedure: The laser energy is applied to the plaques, selectively destroying the abnormal tissue. Local anesthesia is typically applied.
- Advantages: Minimal bleeding, excellent cosmetic results with often less scarring compared to surgery (especially with fractional modes), and precise tissue removal. No sutures are required, ensuring a less invasive experience.
- Considerations: Multiple sessions may be needed for larger or deeper lesions. Post-treatment care involves keeping the treated area clean and protected. Risks include temporary pigmentation changes (hypo- or hyperpigmentation) and, rarely, scarring or infection. It requires a skilled operator.
- Suitability: Effective for lesions of varying sizes, particularly for diffuse plaques where surgical excision might be more challenging, positioning laser treatment as a versatile option.
3. Chemical Peeling (Trichloroacetic Acid – TCA)
TCA is a widely used chemical agent for non-surgical Xanthelasma treatment, often referred to as a chemical peel treatment.
- Procedure: A controlled application of TCA (usually 50-70% concentration) is performed directly onto the Xanthelasma lesions. The acid causes a chemical burn, leading to necrosis of the lipid-laden cells and subsequent peeling.
- Advantages: Non-invasive, relatively inexpensive, and generally provides good cosmetic results. It can be particularly useful for diffuse or multiple small lesions, making it an accessible chemical peel option.
- Considerations: Requires precise application to avoid damage to surrounding healthy skin, especially around the delicate eye area. Multiple sessions are often necessary. Risks include hyperpigmentation (especially in darker skin types), hypopigmentation, scarring, and irritation. Careful post-procedure care to protect the healing skin is essential.
- Suitability: Favored by some for widespread, thinner lesions where surgery might be too aggressive, making it a specific choice for certain types of Xanthelasma.
4. Electrodessication and Curettage (ED&C)
This method involves using an electric current to destroy the Xanthelasma tissue, a form of electrodessication treatment.
- Procedure: A fine needle-like electrode is used to deliver an electric current to the lesion, coagulating and desiccating the tissue. The destroyed tissue is then scraped away with a curette.
- Advantages: Relatively quick, can be performed in an outpatient setting, and effective for many lesions. It offers a swift approach to Xanthelasma removal.
- Considerations: Can cause some temporary redness and swelling. Risk of scarring or pigmentation changes. The control might be less precise than with lasers, potentially leading to more collateral damage if not performed carefully.
- Suitability: Suitable for smaller, raised lesions where this method can be effectively applied.
5. Cryotherapy
This treatment involves freezing the Xanthelasma tissue, often referred to as cryotherapy for Xanthelasma.
- Procedure: Liquid nitrogen is applied to the lesion, typically using a cryospray or cotton-tipped applicator, to freeze and destroy the abnormal cells.
- Advantages: Relatively simple, quick, and non-invasive.
- Considerations: Less precise control compared to surgery or laser. Risk of hypopigmentation (lightening of the skin) due to melanocyte damage, particularly in darker skin types. Multiple sessions might be required, and over-treatment can lead to scarring or tissue damage.
- Suitability: Less commonly favored for Xanthelasma compared to other methods due to the risk of hypopigmentation in a cosmetically sensitive area, but remains an option for select cases where cryotherapy is deemed appropriate.
6. Topical Treatments
While less effective for established Xanthelasma plaques, some experimental or adjunctive topical treatments have been explored.
- Bichloracetic acid (BCA): Similar to TCA but less commonly used for topical treatment.
- Other Topical Agents: Rarely, extremely potent retinoids or other exfoliating agents might be considered for very superficial lesions, but their efficacy is limited for the deeper lipid deposits characteristic of Xanthelasma. Generally, topical creams are not recommended as primary Xanthelasma treatment options due to their limited penetration and potential for irritation without significant therapeutic benefit, making them less viable for comprehensive Xanthelasma removal.
Post-Treatment Care and Recurrence Prevention
Regardless of the chosen Xanthelasma treatment method, proper post-treatment care is vital for optimal healing and minimizing complications. This typically includes keeping the area clean, applying prescribed topical ointments, and protecting the skin from sun exposure. This aftercare is crucial for successful Xanthelasma removal and cosmetic outcome.
Furthermore, patients should be counselled on the importance of managing underlying dyslipidemia, if present. Lifestyle modifications (diet, exercise) and, if necessary, lipid-lowering medications (e.g., statins) can help reduce the risk of new lesion formation or recurrence of Xanthelasma. Regular follow-ups are recommended to monitor for recurrence and overall lipid health, as effective management of underlying conditions can significantly improve long-term outcomes and prevent the return of these eyelid cholesterol deposits.
In summary, the choice of Xanthelasma treatment depends on various factors, including the size, location, and number of lesions, patient preference, and the clinician’s expertise. A consultation with a dermatologist or oculoplastic surgeon is essential to determine the most appropriate and safest approach for individual cases. The primary goal is effective cosmetic removal with minimal scarring and careful consideration of potential underlying systemic health issues, ensuring a holistic approach to managing Xanthelasma.