
Understanding What Does Lupus Rash Look Like Pictures is crucial for early recognition and management of this complex autoimmune condition. The visual manifestations of lupus on the skin are diverse, ranging from mild redness to significant lesions that can cause scarring and disfigurement. This article provides a detailed visual guide and descriptive analysis of the various forms of lupus rash to aid in comprehension.
Lupus rash Symptoms Pictures
Lupus rash symptoms present with a wide array of visual characteristics, making accurate identification of lupus rash symptoms pictures essential for diagnosis. The appearance often depends on the type of cutaneous lupus erythematosus (CLE) and its activity, varying from subtle erythema to severe plaques with atrophy.
Acute Cutaneous Lupus Erythematosus (ACLE)
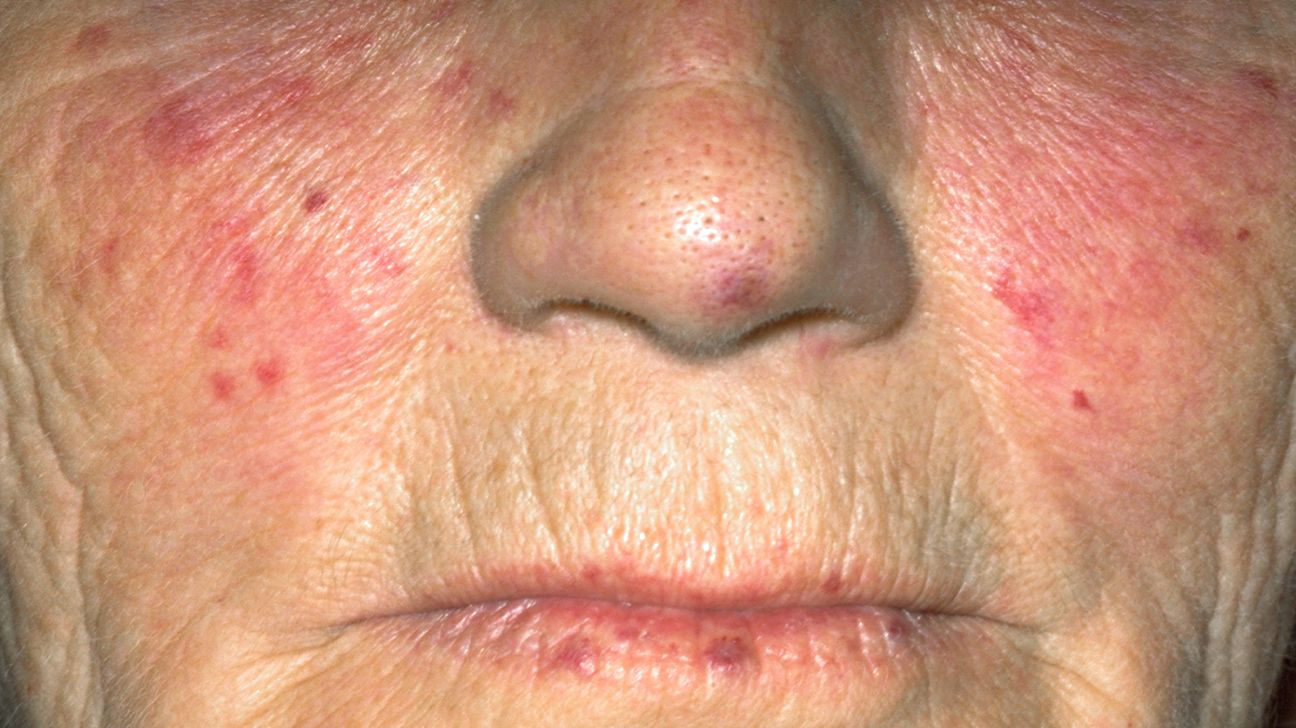
ACLE is frequently associated with systemic lupus erythematosus (SLE) and is characterized by highly photosensitive eruptions. The most iconic form is the malar rash or butterfly rash, which typically covers the cheeks and bridge of the nose, often sparing the nasolabial folds. Key visual symptoms include:
- Malar Rash (Butterfly Rash):
- Intense, red, flat (macular) or slightly raised (papular) patches.
- Symmetrical distribution over the malar eminences and nasal bridge.
- Sharp, well-demarcated borders, resembling a butterfly wing pattern.
- Often feels warm or slightly tender to the touch.
- Exacerbated by sun exposure, leading to increased redness and discomfort.
- Typically does not cause scarring upon resolution.
- Can sometimes extend to the forehead, chin, or ears.
- Generalized Morbilliform Eruption:
- Widespread, measles-like rash, usually red macules and papules.
- Often affects sun-exposed areas but can be more generalized.
- Non-specific in appearance, can be confused with drug eruptions or viral exanthems.
- Pruritic (itchy) or burning sensation may be present.
- Resolves without scarring.
- Commonly appears on the limbs, trunk, and face.

Subacute Cutaneous Lupus Erythematosus (SCLE)
SCLE presents with distinct, non-scarring, photosensitive skin lesions that can be either annular (ring-shaped) or papulosquamous (psoriasiform). These lupus rash symptoms are typically found on sun-exposed areas like the neck, upper chest, back, shoulders, and outer arms, usually sparing the face and knuckles. Visual characteristics include:
- Annular SCLE:
- Red, raised borders with central clearing, forming ring-shaped lesions.
- Lesions can coalesce to form polycyclic patterns.
- Often mistaken for fungal infections or other dermatoses.
- No significant scaling within the center.
- Post-inflammatory hyperpigmentation or hypopigmentation (lightening or darkening of the skin) is common after the rash resolves, but true scarring is rare.
- Can be mildly itchy or asymptomatic.
- Papulosquamous (Psoriasiform) SCLE:
- Red, raised plaques with fine, adherent scales, resembling psoriasis.
- Lesions are well-demarcated.
- Located primarily on sun-exposed areas.
- Can be itchy or feel like a burning sensation.
- Also leaves post-inflammatory pigmentary changes but no scarring.
Chronic Cutaneous Lupus Erythematosus (CCLE)
CCLE encompasses various forms, with discoid lupus erythematosus (DLE) being the most common. These lesions are characterized by their potential to cause permanent scarring and disfigurement. DLE lupus rash symptoms pictures show a distinct and often severe presentation:
- Discoid Lupus Erythematosus (DLE):
- Well-demarcated, coin-shaped (discoid) lesions.
- Typically red to violaceous (purplish) plaques.
- Distinctive features include follicular plugging (keratotic debris within hair follicles), adherent scales, and central atrophy.
- Primarily affects sun-exposed areas, especially the scalp, face (cheeks, nose, ears), neck, and upper trunk, but can appear anywhere.
- On the scalp, DLE causes permanent scarring alopecia (hair loss), where hair follicles are destroyed.
- Lesions often heal with significant scarring, central depression (atrophy), telangiectasias (spider veins), and prominent dyspigmentation (both hyperpigmentation at the edges and hypopigmentation in the center).
- Can be painful, itchy, or have a burning sensation.
- Lupus Profundus (Lupus Panniculitis):
- Deep subcutaneous nodules or plaques.
- Overlying skin may appear normal, red, or show signs of DLE.
- Often found on the arms, shoulders, thighs, and buttocks.
- Heals with significant atrophy and depressions in the skin, often leaving a “cottage cheese” appearance.
- Can be painful or tender.
- Hypertrophic DLE:
- Warty, thick, and verrucous (wart-like) plaques.
- Most commonly seen on the extensor surfaces of the arms, upper back, and face.
- Less common variant of DLE but carries similar scarring potential.
Other Cutaneous Lupus Manifestations
- Bullous Lupus Erythematosus:
- Rare form characterized by tense blisters (bullae) on normal or erythematous skin.
- Often located in sun-exposed areas or areas of trauma.
- Resembles other blistering disorders.
- Heals with milia (small cysts) and hyperpigmentation, but usually minimal scarring unless secondary infection occurs.
- Lupus Vasculitis:
- Inflammation of blood vessels causing palpable purpura (raised, non-blanching red/purple spots), ulcerations, or livedo reticularis (net-like mottled discoloration).
- Can occur on fingers, toes, lower legs, or other areas.
- May lead to gangrene in severe cases.
- Periungual Erythema:
- Redness and swelling around the fingernails, often accompanied by ragged cuticles and nailfold capillary changes (visible under a dermatoscope).
- Oral Ulcers:
- Painless or mildly painful sores on the palate, buccal mucosa, or tongue.
- Often red with a white border.
- Can be a significant diagnostic clue.
Signs of Lupus rash Pictures
Identifying the distinct signs of lupus rash pictures is crucial for differentiating it from other dermatological conditions. The visual cues extend beyond mere redness, involving specific patterns, textures, and associated features that are indicative of lupus activity. These signs often guide clinicians towards an accurate diagnosis of the various lupus rash types.
Distinguishing Features of ACLE Rash
The malar rash, a hallmark of ACLE and often of systemic lupus erythematosus (SLE), exhibits specific signs:
- Symmetry and Distribution: The classic “butterfly” pattern is highly symmetrical, covering the cheeks and nose. The unique sparing of the nasolabial folds (grooves from the nose to the corners of the mouth) is a key diagnostic sign that helps distinguish it from rosacea or seborrheic dermatitis.
- Erythema: The redness is typically bright, vivid, and continuous across the affected areas. It can intensify with sun exposure, stress, or fever.
- Edema: A subtle swelling or puffiness often accompanies the redness, making the lesions slightly raised to the touch.
- Texture: The skin usually remains smooth or mildly scaly, without significant induration or thickening. There is no significant follicular plugging or atrophy in ACLE lesions.
- Photosensitivity: A strong history of the rash appearing or worsening after sun exposure is a primary sign. This photosensitive rash is a significant indicator of lupus.
Characteristic Signs of SCLE Rash
SCLE presents with two main morphological patterns, each with distinct signs:
- Annular Pattern Signs:
- Ring-Shaped Lesions: The most striking sign is the formation of circular or arcuate (C-shaped) lesions with raised, erythematous borders and central clearing.
- Polycyclic Confluence: Individual rings can merge, creating larger, serpiginous (snake-like) or polycyclic patterns. This extensive skin rash lupus can be quite visually complex.
- Fine Scale: A delicate, non-adherent scale may be present, particularly on the leading edge of the lesions.
- Absence of Scarring: While post-inflammatory dyspigmentation (both hyper- and hypopigmentation) is common upon resolution, true scarring, atrophy, or follicular plugging are notably absent. This is a critical differentiating factor from DLE.
- Photosensitive Distribution: The lesions typically appear on sun-exposed areas like the V-neck area of the chest, upper back, shoulders, and extensor aspects of the arms, sparing the face in many cases.
- Papulosquamous (Psoriasiform) SCLE Signs:
- Psoriasiform Plaques: Resembles psoriasis with erythematous, scaly plaques. The scales are often finer and less silvery than classic psoriasis.
- Well-Demarcated: Lesions typically have distinct, clear borders.
- Similar Distribution: Like annular SCLE, these also favor sun-exposed body parts.
Key Signs of DLE Rash (Chronic Cutaneous Lupus)
DLE lesions exhibit specific and often permanent signs:
- Coin-Shaped Plaques: The characteristic discoid shape is a primary sign, presenting as round or oval lesions.
- Erythema and Induration: Lesions are red to violaceous and feel firm or hardened (indurated) to the touch due to inflammation and fibrosis.
- Follicular Plugging: A hallmark sign, visible as keratinous plugs within the dilated hair follicles at the surface of the lesion, giving a “carpet tack” appearance when removed.
- Adherent Scale: A tightly adherent, often thick, scale covers the surface of the plaque.
- Central Atrophy: As lesions mature, the center often becomes depressed, thin, and smooth due to destruction of collagen and elastin. This scarring atrophy is permanent.
- Dyspigmentation: Highly characteristic are the pigmentary changes: hypopigmentation (loss of pigment, appearing white) in the atrophic center and hyperpigmentation (darkening) at the periphery of the lesion.
- Alopecia (Scalp): On the scalp, DLE causes irreversible patchy hair loss with scarring, leaving shiny, bald areas where follicles have been destroyed. This is a critical sign of DLE.
- Telangiectasias: Small, dilated blood vessels (spider veins) are often visible within and around the lesions, especially in atrophic areas.
Other Important Lupus Skin Signs
- Mucosal Ulcers: Painless or mildly painful ulcers in the mouth (palate, buccal mucosa) or nose are common. These are often red at the base with a whitish rim.
- Periungual Erythema and Capillary Changes: Redness around the nailfolds, sometimes with telangiectasias and visible capillary loops (seen with a dermatoscope), are signs of microvascular involvement.
- Livedo Reticularis: A mottled, purplish, net-like discoloration of the skin, particularly on the legs, arms, and trunk, can indicate vascular involvement.
- Raynaud’s Phenomenon: Though not a rash, this vasospastic condition causes episodic blanching (white), cyanosis (blue), and then erythema (red) of the fingers and toes, often triggered by cold or stress, and is frequently associated with lupus.
Early Lupus rash Photos
Recognizing early lupus rash photos can significantly impact the speed of diagnosis and initiation of treatment, potentially preventing progression and long-term complications. The initial presentation of lupus on the skin can be subtle and non-specific, often mistaken for more common dermatological issues. Early signs of lupus rash may be transient or appear as mild erythema before developing into more characteristic lesions. Awareness of these initial visual clues is vital for timely intervention.
Initial Manifestations of ACLE
The earliest signs of acute cutaneous lupus erythematosus often involve heightened sensitivity to sunlight:
- Subtle Erythema: The very first indication might be a mild, transient redness on sun-exposed skin, particularly on the face (cheeks and nose) after sun exposure. This redness may fade quickly.
- Mild Photosensitivity Reaction: Patients may report unusual or exaggerated sunburn-like reactions with minimal sun exposure, characterized by redness, mild swelling, and warmth. This “photosensitive rash” is a key early indicator.
- Faint Malar Flush: Before the classic butterfly rash fully develops, there might be a symmetrical, pinkish-red flush across the malar eminences, often mistaken for blushing or mild rosacea. It lacks the sharp demarcation of a fully developed malar rash.
- Sparse Morbilliform Spots: A few scattered, small, red macules or papules, resembling a mild viral rash, may appear on the trunk or limbs, particularly in sun-exposed areas. These can be transient and easily overlooked.
- Mild Itching or Burning Sensation: Some individuals might experience a subtle itchy or burning sensation on the affected skin, preceding visible changes or accompanying mild erythema.
Incipient SCLE Lesions
Early SCLE typically begins on sun-exposed areas, sometimes with vague symptoms:
- Small Erythematous Papules: The onset often involves small, slightly raised, red bumps, usually found on the upper back, shoulders, or chest.
- Patchy Redness: Irregular patches of redness, often accompanied by a mild, fine scale, may be observed on the arms or décolletage. These early skin rash lupus patches might not yet show the characteristic annular or psoriasiform patterns.
- Increased Skin Sensitivity: The skin in affected areas might feel more sensitive or reactive to touch or light friction, even before distinct lesions appear.
- Asymptomatic Onset: Importantly, early SCLE lesions can sometimes be entirely asymptomatic, with no itching or pain, leading to delayed recognition.
Beginning Stages of DLE
Discoid lupus erythematosus often starts subtly but can progress to significant damage:
- Small Erythematous Papules or Plaques: The earliest DLE lesion may manifest as a small, slightly raised, reddish papule or plaque. It might initially resemble a common bug bite or a minor skin irritation.
- Faint Scaling: A very fine, thin scale might be present on the surface of these early lesions, which might not yet be adherent or show follicular plugging.
- Mild Itching or Discomfort: Initial DLE lesions can be mildly itchy or cause a vague sensation of discomfort.
- Localized Hair Loss (Scalp): On the scalp, one of the earliest signs can be a small patch of hair thinning or loss, often accompanied by mild redness. This can be mistaken for common alopecia. Closer inspection might reveal subtle follicular plugs or early signs of scarring.
- Limited Distribution: Initially, there may be only one or a few lesions, often on the face (ears, cheeks), scalp, or neck. They are not yet widespread.
- Progressive Induration: Over weeks to months, these early lesions gradually become more firm and indurated, and the characteristic features of follicular plugging, adherent scale, and central atrophy begin to develop. These are critical early lupus rash photos that show evolution.
Other Early Skin Changes Associated with Lupus
- Recurrent Oral Sores: While often painless, recurrent small sores inside the mouth (on the palate or cheeks) can be one of the earliest non-rash skin manifestations of lupus.
- Raynaud’s Phenomenon Onset: New onset of Raynaud’s phenomenon, where fingers or toes become white, then blue, then red in response to cold or stress, can be an early warning sign of underlying autoimmune disease, including lupus.
- Unexplained Photosensitivity: Any new or increased sensitivity to sunlight resulting in disproportionate skin reactions should prompt consideration of lupus, even if a classic rash hasn’t developed.
Early recognition necessitates a high index of suspicion, especially in individuals with other systemic symptoms or a family history of autoimmune diseases. Any persistent, unusual, or sun-sensitive skin changes warrant medical evaluation for potential lupus rash.
Skin rash Lupus rash Images
Detailed examination of skin rash lupus rash images reveals the vast phenotypic spectrum of cutaneous lupus erythematosus. These images are invaluable for understanding the specific visual cues that characterize each type of lupus skin involvement, from acute photosensitive eruptions to chronic scarring lesions. Grasping these visual details is fundamental for accurate diagnosis and management.
Acute Cutaneous Lupus Erythematosus (ACLE) Visuals
ACLE photos illustrate transient, highly photosensitive rashes:
- Malar Rash Imagery:
- Classic Butterfly Shape: Vivid red, confluent erythema covering the malar eminences and nasal bridge. Crucially, the nasolabial folds typically remain clear, creating a distinct “butterfly” outline.
- Erythematous Macules and Papules: Smooth to slightly elevated lesions that are often warm to the touch. The redness is typically bright and uniform across the affected area.
- Sun-Induced Flare: Images often depict the malar rash intensifying immediately after sun exposure, highlighting its photosensitive nature.
- Absence of Scarring: Clear images show resolution without any textural changes, scarring, or atrophy, distinguishing it from other chronic forms.
- Generalized Morbilliform Eruption Visuals:
- Widespread Maculopapular Rash: Resembles a measles-like eruption with numerous small, red, flat (macular) or slightly raised (papular) lesions scattered over the trunk, limbs, and face.
- Non-Specific Appearance: Images highlight the challenge in differentiating this from drug reactions or viral exanthems without further context.
- Variable Intensity: The rash can range from faint pink to intense red, and may be itchy.
Subacute Cutaneous Lupus Erythematosus (SCLE) Visuals
SCLE images display distinctive non-scarring, photosensitive lesions:
- Annular SCLE Lesion Photos:
- Ring-Shaped or Arciform Patches: Clear images of erythematous plaques with active, raised borders and characteristic central clearing. The rings can be singular or coalesce into polycyclic patterns.
- Fine Peripheral Scaling: A subtle, thin, non-adherent scale may be visible along the raised edge of the lesions.
- Distribution on Sun-Exposed Skin: Photos consistently show these lesions on the V-neck area, shoulders, upper back, and extensor surfaces of the arms, sparing the hands and face in many cases.
- Post-inflammatory Pigmentary Changes: Images frequently show areas of hypopigmentation (lightening) or hyperpigmentation (darkening) in the areas where lesions have resolved, without true epidermal or dermal atrophy.
- Papulosquamous (Psoriasiform) SCLE Images:
- Plaque-like Lesions with Scales: Visuals of well-demarcated, red plaques covered with fine, often whitish, scales. These bear a striking resemblance to psoriasis.
- Similar Distribution to Annular Form: Located in typical SCLE sun-exposed areas.
Chronic Cutaneous Lupus Erythematosus (CCLE) Visuals
CCLE images depict lesions with a high potential for scarring and permanent changes:
- Discoid Lupus Erythematosus (DLE) Photos:
- Well-Demarcated Erythematous Plaques: Images clearly show round or oval, reddish-purple plaques with distinct borders.
- Follicular Plugging: Close-up views reveal characteristic keratinous plugs within the hair follicles on the lesion surface, a key diagnostic sign.
- Adherent Scaling: Thick, tightly attached scales are visible, sometimes making the lesion appear rough or crusted.
- Central Atrophy and Scarring: Pictures often display depressed, smooth, shiny, and thin skin in the center of older lesions due to dermal atrophy and fibrosis.
- Dyspigmentation: Striking contrast between hypopigmented (whitened) centers and hyperpigmented (darkened) borders is a classic visual.
- Scalp DLE and Scarring Alopecia: Images of the scalp show patchy, irregular areas of permanent hair loss with shiny, atrophic skin, indicating irreversible follicular destruction.
- Ear Involvement: DLE commonly affects the ear conchae, leading to painful lesions, cartilage destruction, and disfigurement.
- Lupus Profundus (Panniculitis) Visuals:
- Subcutaneous Nodules and Depressions: Images show deep, firm nodules that may or may not have overlying skin changes. Upon resolution, characteristic deep depressions and subcutaneous atrophy are visible, creating an uneven skin contour.
- Pain and Tenderness: While not visible, this is an important clinical association.
Less Common but Significant Lupus Skin Visuals
- Bullous Lupus Erythematosus Pictures:
- Tense Blisters (Bullae): Images show fluid-filled blisters on erythematous or normal-appearing skin, often in sun-exposed or traumatized areas.
- Healing with Milia and Pigmentation: After rupture, lesions heal with small white cysts (milia) and dark spots, typically without significant scarring.
- Lupus Vasculitis Images:
- Palpable Purpura: Visible as raised, red-to-purple, non-blanching spots, often on the lower legs or fingers, indicating inflammation of small blood vessels.
- Ulcerations: Images may show skin breakdown and chronic sores resulting from severe vascular damage.
- Livedo Reticularis: A striking, net-like, bluish-red mottled pattern on the skin, especially on the extremities, suggesting impaired blood flow.
- Oral Ulcers Visuals:
- Painless White-Rimmed Red Sores: Images show discrete ulcers on the hard palate, buccal mucosa, or gums, typically surrounded by a white or reddish halo.
- Periungual Erythema and Capillary Changes:
- Redness Around Nails: Visible erythema and swelling of the skin folds around the fingernails.
- Telangiectasias: Fine, dilated blood vessels at the nail folds.
These detailed visual descriptions enhance the understanding of what does lupus rash look like pictures across its diverse presentations, aiding both patients and clinicians in recognizing and classifying these complex skin manifestations.
Lupus rash Treatment
Effective lupus rash treatment is multi-faceted, aiming to control inflammation, prevent new lesions, minimize scarring, alleviate symptoms, and improve quality of life. The approach is tailored to the type and severity of the cutaneous lupus, as well as the presence of systemic involvement. A comprehensive treatment plan often combines topical, intralesional, and systemic therapies, alongside crucial lifestyle modifications for managing a chronic skin rash lupus.
Topical and Intralesional Therapies
These treatments are usually the first-line for localized or less severe lupus rashes, especially for DLE and some SCLE lesions.
- Topical Corticosteroids:
- Mechanism: Potent anti-inflammatory and immunosuppressive effects.
- Application: High-potency corticosteroids (e.g., clobetasol, halobetasol) are applied directly to the lesions. Mid-potency steroids may be used for less severe or sensitive areas (e.g., face).
- Usage: Applied once or twice daily for limited periods to avoid side effects like skin thinning (atrophy), telangiectasias, and hypopigmentation.
- Effectiveness: Highly effective in reducing redness, scaling, and inflammation in discoid and subacute lesions.
- Intralesional Corticosteroids:
- Mechanism: Direct injection of corticosteroids (e.g., triamcinolone acetonide) into stubborn, thickened lesions.
- Usage: Particularly useful for hypertrophic DLE, thick DLE plaques, or lupus profundus nodules that do not respond to topical agents.
- Advantages: Delivers high concentrations of medication directly to the site of inflammation, reducing systemic absorption and side effects.
- Frequency: Injections are typically administered every 3-4 weeks until lesions improve.
- Topical Calcineurin Inhibitors:
- Mechanism: Immunomodulating agents (e.g., tacrolimus, pimecrolimus) that suppress inflammation without the side effects of steroids.
- Usage: Used for facial lupus rashes or in areas where prolonged steroid use is undesirable. Can be a steroid-sparing option for mild to moderate lesions.
- Advantages: Does not cause skin atrophy.
Systemic Medications
Systemic therapies are employed for widespread, severe, or refractory cutaneous lupus, or when there is concurrent systemic lupus erythematosus (SLE) activity.
- Antimalarials:
- Hydroxychloroquine (Plaquenil): The cornerstone of lupus rash treatment.
- Mechanism: Modulates immune response, reduces photosensitivity, and stabilizes lysosomal membranes.
- Usage: Effective for ACLE, SCLE, and DLE. Often used long-term.
- Dosage: Typically 200-400 mg daily.
- Side Effects: Generally well-tolerated; rare but serious side effect is retinal toxicity, requiring regular ophthalmologic screening.
- Chloroquine: Similar to hydroxychloroquine but with a higher risk of ocular toxicity.
- Quinacrine: Can be added to hydroxychloroquine or chloroquine for refractory cases. It does not have retinal toxicity but can cause yellow skin discoloration.
- Hydroxychloroquine (Plaquenil): The cornerstone of lupus rash treatment.
- Systemic Corticosteroids:
- Mechanism: Potent anti-inflammatory and immunosuppressive.
- Usage: Used for severe, widespread, or rapidly progressing lupus rashes, or for severe systemic manifestations. Usually prescribed as a short course or tapered to the lowest effective dose.
- Side Effects: Numerous side effects with long-term use (e.g., weight gain, osteoporosis, hypertension, diabetes), limiting prolonged high-dose therapy.
- Immunosuppressants/Immunomodulators:
- Methotrexate:
- Mechanism: Folic acid antagonist, suppressing immune cell proliferation.
- Usage: Effective for refractory SCLE and DLE, especially when antimalarials are insufficient.
- Administration: Weekly oral or subcutaneous doses.
- Side Effects: Nausea, fatigue, liver toxicity, bone marrow suppression; requires regular monitoring.
- Azathioprine (Imuran):
- Mechanism: Inhibits purine synthesis, thus immune cell proliferation.
- Usage: For severe or widespread cutaneous lupus unresponsive to antimalarials and methotrexate.
- Side Effects: Nausea, bone marrow suppression, liver toxicity; requires regular blood monitoring.
- Mycophenolate Mofetil (CellCept):
- Mechanism: Inhibits inosine monophosphate dehydrogenase, suppressing lymphocyte proliferation.
- Usage: Effective for various forms of cutaneous lupus, particularly DLE and bullous lupus.
- Side Effects: Gastrointestinal upset, bone marrow suppression, increased infection risk.
- Thalidomide:
- Mechanism: Immunomodulatory and anti-inflammatory effects.
- Usage: Reserved for very severe, refractory DLE and SCLE due to significant side effects.
- Side Effects: Severe teratogenicity (birth defects), peripheral neuropathy; requires strict monitoring and risk management programs.
- Dapsone:
- Mechanism: Anti-inflammatory and inhibits neutrophil function.
- Usage: Useful for bullous lupus and sometimes for urticarial vasculitis of lupus.
- Side Effects: Hemolysis (especially in G6PD deficient patients), methemoglobinemia; requires baseline G6PD testing.
- Methotrexate:
- Biologics:
- Belimumab (Benlysta):
- Mechanism: A B-lymphocyte stimulator (BLyS) protein inhibitor, reducing B-cell survival.
- Usage: Approved for SLE, including its cutaneous manifestations, particularly ACLE and SCLE.
- Administration: Intravenous or subcutaneous.
- Side Effects: Infusion reactions, increased infection risk.
- Rituximab (Rituxan):
- Mechanism: Chimeric monoclonal antibody targeting CD20 on B-lymphocytes.
- Usage: Off-label for refractory severe cutaneous lupus, particularly when associated with severe systemic disease.
- Side Effects: Infusion reactions, increased infection risk, progressive multifocal leukoencephalopathy (PML) rare.
- Belimumab (Benlysta):
Ancillary Treatments and Lifestyle Modifications
These measures are fundamental for all patients with lupus rash to prevent flares and minimize damage.
- Sun Protection:
- Daily Sunscreen Use: Broad-spectrum sunscreen with SPF 30 or higher, applied generously and reapplied every 2 hours, even on cloudy days.
- Protective Clothing: Wearing wide-brimmed hats, UV-protective clothing, and sunglasses.
- Sun Avoidance: Limiting outdoor activities during peak UV hours (10 AM to 4 PM).
- Window Films: Using UV-protective films on home and car windows.
- Importance: Essential for preventing the exacerbation of photosensitive lupus rashes and is a cornerstone in managing skin rash lupus.
- Smoking Cessation:
- Impact: Smoking can worsen cutaneous lupus, reduce the effectiveness of antimalarial medications, and delay healing.
- Recommendation: Strong recommendation for all patients to stop smoking.
- Scar Management (for DLE):
- Cosmetic Interventions: For residual scarring, atrophy, or dyspigmentation from DLE, options include laser therapy (for redness, pigmentation, or texture), microdermabrasion, dermal fillers (for atrophic scars), and surgical revision.
- Camouflage Makeup: Helps cover disfiguring lesions or pigmentary changes.
- Regular Skin Examination:
- Self-Checks: Patients should regularly examine their skin for new or changing lesions.
- Dermatologist Visits: Routine follow-ups with a dermatologist are crucial for monitoring existing lesions, identifying new ones, and adjusting treatment.
- Emotional Support: Managing a visible skin condition like lupus rash can significantly impact mental well-being. Support groups, counseling, and psychological therapies can be beneficial.
The choice of lupus rash treatment depends on various factors, including the specific type of cutaneous lupus, its extent, impact on quality of life, patient comorbidities, and response to previous therapies. A collaborative approach between the patient, dermatologist, and rheumatologist is essential for optimizing outcomes and ensuring comprehensive care for these complex skin manifestations.