
When considering What Does A Hernia Look Like Symptoms Pictures, it’s crucial to understand that hernias manifest as visible bulges or swellings, often accompanied by distinct physical sensations. These visual cues and symptomatic experiences are key to identification and understanding the condition.
Hernia Symptoms Pictures
Hernias primarily present as a noticeable bulge or lump beneath the skin, the appearance of which can vary significantly depending on the type, size, and location of the hernia. While some hernias are small and barely perceptible, others can grow quite large, causing considerable cosmetic distortion and discomfort. The visual manifestation of a hernia is often a primary indicator for individuals seeking medical attention, and understanding these visual symptoms is key.
Key visual characteristics to observe when examining what a hernia looks like include:
- Location of the Bulge:
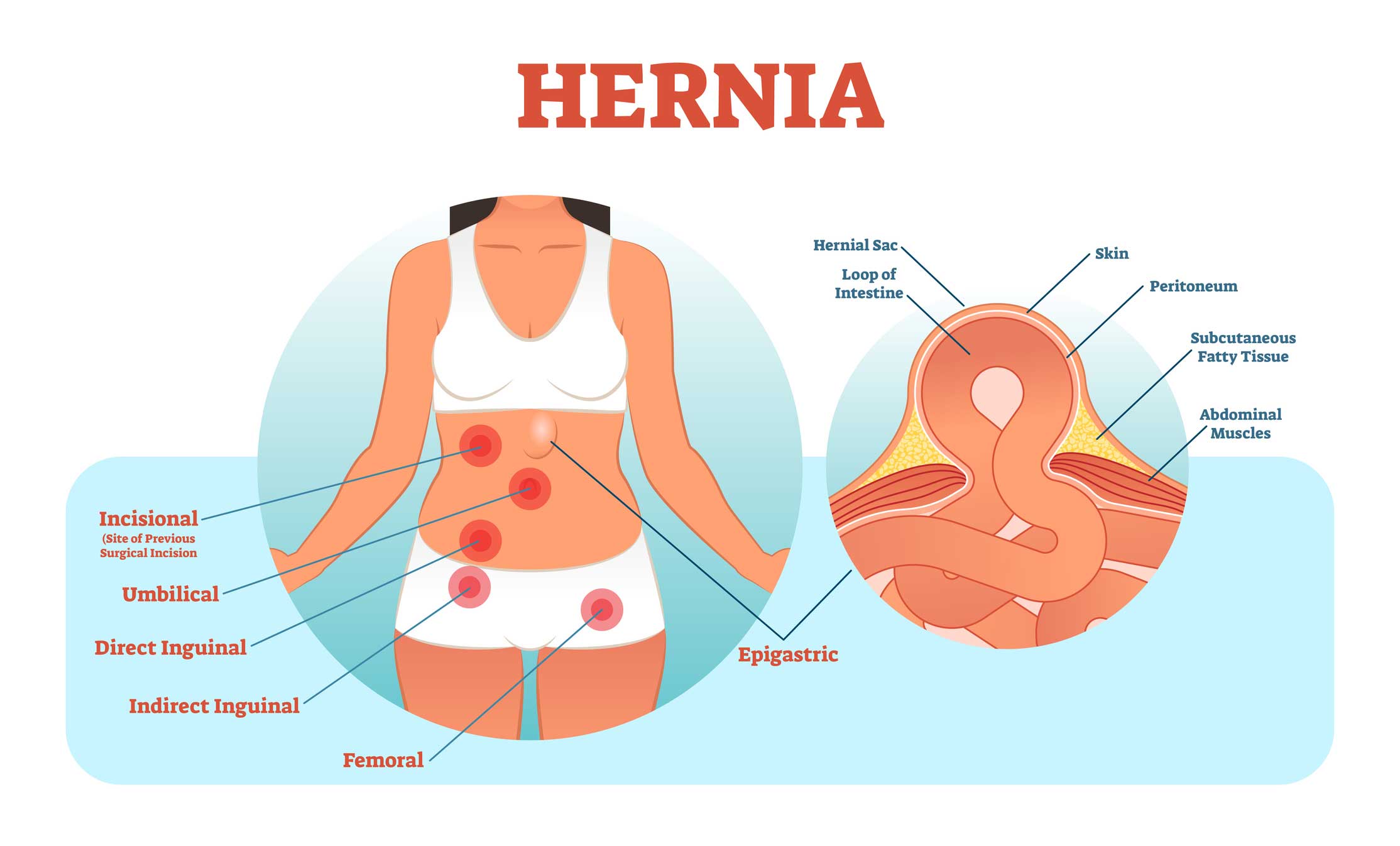
- Inguinal Hernia: Typically appears in the groin area, either on one side or both. In men, it can extend into the scrotum, causing scrotal swelling. The bulge is usually most prominent when standing, coughing, or straining.
- Femoral Hernia: Less common, often seen just below the groin crease, near the upper thigh. It tends to be smaller and rounder than an inguinal hernia.
- Umbilical Hernia: Manifests as a bulge around or in the belly button (navel). It’s common in infants but can occur in adults, often becoming more noticeable with increased abdominal pressure.
- Incisional Hernia: Develops at the site of a previous surgical incision, appearing as a bulge along or near the scar. Its size and shape are highly variable, often mirroring the underlying defect in the abdominal wall.
- Epigastric Hernia: Located in the midline of the abdomen, between the belly button and the breastbone (sternum). These are often small and can sometimes be felt rather than clearly seen initially.
- Spigelian Hernia: Occurs along the outer edge of the rectus abdominis muscle, typically below the level of the navel. These are often difficult to diagnose visually as they can be situated within the abdominal muscle layers.
- Parastomal Hernia: Appears around an ostomy (stoma) site, such as a colostomy or ileostomy, as a bulge adjacent to the stoma.
- Size and Shape:
- Hernias can range from a pea-sized lump to a grapefruit-sized mass.
- The shape can be rounded, oval, or irregular, depending on the contents protruding and the defect’s geometry.
- A reducible hernia may disappear or decrease in size when the person lies down or if gently pushed back into the abdomen.
- An irreducible or incarcerated hernia will remain prominent and cannot be pushed back.
- Texture and Consistency:
- Often soft and doughy to the touch, indicating fat or intestine.
- Can feel firm or tense, especially if incarcerated or strangulated, which is a medical emergency.
- A gurgling sensation or sound may be felt when manipulating the bulge, indicating bowel contents.
- Color and Skin Changes:
- Typically, the skin over a hernia bulge appears normal in color.
- However, in cases of inflammation, incarceration, or strangulation, the overlying skin may become red, purplish, or discolored.
- The skin may appear stretched, thin, or shiny over a large, long-standing hernia.
- Chronic irritation or friction in skin folds created by large hernias can lead to redness, chafing, or even fungal infections.
- Dynamic Appearance:
- The bulge often becomes more pronounced with activities that increase intra-abdominal pressure.
- These activities include coughing, sneezing, straining during bowel movements, lifting heavy objects, or prolonged standing.
- Conversely, the bulge may recede or disappear when lying down or relaxing abdominal muscles.
Accompanying symptoms that are often felt, rather than seen, include:
- Pain or Discomfort:
- A dull ache or a heavy sensation in the area of the bulge.
- Pain that worsens with activity and improves with rest.
- Sharp, sudden pain if the hernia becomes incarcerated or strangulated.
- A burning or tingling sensation, particularly in inguinal hernias, due to nerve irritation.
- Generalized abdominal discomfort or pressure, especially with large hernias.
- Pressure Sensation: A feeling of fullness or dragging in the affected area.
- Weakness: A feeling of weakness or pressure in the groin, thigh, or abdominal wall.
- Digestive Issues: In some cases, particularly with large hernias affecting the bowel, there might be constipation or changes in bowel habits.
Observing these visual and symptomatic details is critical for an accurate assessment of a potential hernia. Always seek medical advice for proper diagnosis and treatment planning.

Signs of Hernia Pictures
The visual “signs of hernia” refer to the observable characteristics that betray the presence of this condition, often becoming more evident as the hernia progresses or under specific circumstances. These signs are what medical professionals and individuals look for to confirm a suspected hernia. Beyond the basic bulge, there are nuances in how these signs present, providing clues about the hernia’s type and severity.
Detailed signs of a hernia that would be captured in pictures include:
- Visible Protrusion Under the Skin:
- Dynamic Bulge: The most defining sign is a protrusion that appears or becomes more prominent when the patient stands, coughs, laughs, strains, or performs activities that increase abdominal pressure. This dynamic appearance is a strong diagnostic indicator.
- Static Bulge (Irreducible): If the bulge remains visible regardless of position or activity and cannot be gently pushed back, it indicates an irreducible or incarcerated hernia, which is a more serious condition.
- Asymmetry: For most hernias, especially inguinal and femoral, the bulge appears on one side, creating an asymmetry in the body region (e.g., one side of the groin or abdomen appears swollen).
- Changes in Skin Texture and Appearance Over the Bulge:
- Stretched or Thinned Skin: Over time, a large, chronic hernia can cause the overlying skin to become noticeably stretched, thinner, and sometimes shiny due to constant tension. This can reveal the contours of the underlying protrusion more clearly.
- Discoloration (in complications): In cases of incarceration or strangulation, the skin over the hernia sac may exhibit significant discoloration. This can range from erythema (redness) due to inflammation, to a purplish or bluish hue indicating compromised blood supply (ischemia or necrosis). This is a critical sign of a medical emergency.
- Edema and Swelling: Beyond the primary bulge, localized swelling and edema of the surrounding tissues may occur, particularly if there’s inflammation or lymphatic obstruction.
- Visible Venous Engorgement: In some long-standing or very large hernias, the veins under the skin might become more prominent or engorged, especially if there’s pressure on venous return.
- Palpable Signs (What you’d feel if you touched a picture):
- “Impulse on Cough”: When a finger is placed over the hernia defect, a distinct impulse or thrust can be felt when the patient coughs. This sign confirms that abdominal contents are pushing through the weakened area.
- Tenderness: Localized tenderness or pain upon palpation over the hernia site is a common sign, indicating nerve irritation or inflammation. Severe tenderness suggests incarceration or strangulation.
- Rigidity or Firmness: While many hernias are soft, an incarcerated hernia can feel firm or rigid due to trapped contents, which cannot be reduced. This rigidity, especially if accompanied by severe pain, is an alarming sign.
- Crepitation: In rare cases, if gas is trapped within the hernia sac (e.g., from bowel perforation), a crackling sensation (crepitation) might be felt.
- Associated Symptoms Indicating Complications:
- Sudden, Severe Pain: A dramatic increase in pain, especially if it becomes constant and sharp, is a strong indicator of incarceration or strangulation.
- Nausea and Vomiting: These gastrointestinal symptoms, particularly if combined with severe pain and a firm, irreducible bulge, point towards bowel obstruction due to strangulation.
- Fever: The presence of fever along with a painful, discolored hernia suggests an inflammatory or infectious process, potentially due to strangulation and tissue death.
- Changes in Bowel Habits: Constipation, inability to pass gas, or abdominal distension can be signs of bowel obstruction related to an incarcerated hernia.
Understanding these comprehensive signs allows for a more informed assessment when reviewing “signs of hernia pictures,” helping to differentiate between simple reducible hernias and those requiring urgent medical intervention. Early recognition of these signs is paramount for preventing serious complications.
Early Hernia Photos
Early hernia manifestations can be subtle, often beginning as minor discomfort or a barely perceptible lump that might go unnoticed until it becomes more pronounced. “Early hernia photos” would capture these initial, less obvious stages, highlighting the importance of vigilance even for minimal symptoms. The appearance in the early stages can be quite different from a fully developed hernia, making early detection challenging but crucial for simpler treatment outcomes.
Key aspects that “early hernia photos” would illustrate:
- Small, Intermittent Protrusions:
- Barely Visible Bulge: Initially, the hernia may appear as a very small, soft swelling that is only visible when standing, coughing, or straining. It often disappears completely when lying down or relaxing.
- Fluctuating Presence: The bulge might not be present all the time, appearing and disappearing, which can lead individuals to dismiss it as insignificant. Early photos often show the patient in positions that elicit the bulge.
- Localized to the Defect: The early lump is usually quite localized to the actual area of weakness in the muscle or fascial wall, such as the internal ring for inguinal hernias, or a tiny spot near the navel for umbilical hernias.
- Subtle Skin Changes:
- Normal Skin Color and Texture: In the very early stages, the overlying skin typically shows no signs of discoloration, stretching, or inflammation. It appears completely normal.
- No Significant Edema: There is usually no associated swelling or fluid retention in the surrounding tissues.
- Mild Discomfort and Sensations:
- Dull Ache or Pressure: Rather than sharp pain, early hernias often present with a vague feeling of discomfort, pressure, or a dull ache in the affected area, especially after physical activity or prolonged standing.
- Feeling of Heaviness: A sensation of heaviness or a “pulling” feeling in the groin or abdomen might be reported before a visible lump is consistently present.
- Burning or Tingling (early nerve irritation): Sometimes, nerve irritation can be an early symptom, manifesting as a mild burning or tingling sensation in the region even before a prominent bulge is felt or seen.
- Cough Impulse without Clear Bulge: In some very early inguinal hernias, a physician might be able to feel a cough impulse during examination even if a visible bulge isn’t apparent to the patient.
- Differentiation from Other Lumps:
- Lipomas: Early hernias can sometimes be mistaken for benign fatty lumps (lipomas). However, hernias typically have a cough impulse and reducibility, which lipomas do not.
- Lymph Nodes: Swollen lymph nodes can occur in the groin (inguinal lymphadenopathy) but are usually firmer, less mobile, and don’t typically reduce or have a cough impulse.
- Cysts: Sebaceous cysts or other benign cysts are usually fixed to the skin and lack the dynamic nature of a hernia.
- Muscle Strains: Muscular strains cause pain, but typically no distinct lump or bulge, unless there is a hematoma.
Identifying these early signs through careful observation and awareness of subtle physical changes is vital. An “early hernia photo” collection would serve to educate individuals on what to look for, encouraging prompt medical evaluation before the condition progresses to a more complicated state requiring more invasive intervention. It’s crucial to remember that even a small, reducible bulge, especially if accompanied by discomfort, warrants medical attention to prevent potential growth and complications.
Skin rash Hernia Images
While a hernia itself is not a skin disease, its presence, particularly when large or complicated, can lead to various secondary skin conditions or “skin rash hernia images” that are important to recognize. These skin manifestations are often a result of mechanical factors, inflammation, or compromised circulation, offering critical visual clues about the hernia’s status and potential complications. Understanding these skin-related issues is particularly relevant for a website focusing on skin disease symptoms.
Detailed descriptions of skin changes and rashes associated with hernias:
- Erythema (Redness) and Inflammation:
- Local Inflammation: The skin directly overlying an incarcerated or strangulated hernia will often become visibly red, warm to the touch, and swollen. This erythema is a direct sign of inflammation within the hernia sac or compromised tissue.
- Diffuse Redness: In severe cases of strangulation, the redness might spread beyond the immediate hernia site, indicating a more widespread inflammatory response or cellulitis.
- Skin Irritation from Friction: Large hernias, especially in skin folds (e.g., groin, abdominal pannus), can cause skin-on-skin friction, leading to intertrigo – a red, inflamed rash that can be painful and itchy.
- Discoloration Indicating Ischemia or Necrosis:
- Purplish or Bluish Hue: This is a critical sign of a strangulated hernia. The purplish or bluish discoloration signifies venous congestion and subsequent arterial compromise, leading to ischemia (lack of blood flow) and potential necrosis (tissue death) of the entrapped bowel or omentum. This is an absolute medical emergency.
- Darkening and Necrotic Patches: As tissue death progresses, the skin can become darker, almost black, and may show signs of blistering or ulceration. This indicates a severe and advanced stage of strangulation requiring immediate surgical intervention.
- Skin Thinning and Stretching:
- Shiny Appearance: Over a long-standing, large hernia, the constant tension and stretching can cause the skin to thin and appear shiny, almost translucent, revealing underlying vascular patterns more distinctly.
- Striae (Stretch Marks): Rapid growth of a hernia, similar to rapid weight gain or pregnancy, can lead to the formation of striae or stretch marks over the bulging area. These typically start as reddish or purplish lines and fade to white or silver over time.
- Maceration and Secondary Infections:
- Moisture and Maceration: Large abdominal or groin hernias can create deep skin folds where moisture can accumulate. This leads to maceration, characterized by softened, whitish, and fragile skin.
- Fungal Infections (Candidiasis): Macerated skin folds are highly susceptible to fungal infections, particularly candidiasis. These appear as bright red rashes with satellite lesions (smaller spots nearby) and often involve itching, burning, and sometimes a foul odor.
- Bacterial Infections: Skin breakdown from maceration or chronic irritation can also lead to secondary bacterial infections, manifesting as pustules, crusting, or worsening redness and tenderness.
- Ulceration: In rare severe cases, especially with persistent pressure or neglect, the stretched and compromised skin over a very large hernia can ulcerate, creating open sores that are prone to infection and difficult to heal.
- Surgical Scar-Related Issues (for incisional/parastomal hernias):
- Redness and Swelling Around the Scar: For incisional hernias, redness and swelling will typically appear around the surgical scar, indicating the underlying defect.
- Scar Discoloration/Hypertrophy: While not a “rash,” the appearance of the scar itself can be affected, potentially becoming hypertrophic (raised) or keloidal, especially if there’s chronic tension from the hernia.
- Stoma Site Irritation (Parastomal Hernias): For parastomal hernias, the skin around the stoma and adjacent to the hernia can become irritated, inflamed, or exhibit a rash due to leakage from the stoma or friction from appliances, sometimes exacerbating the hernia’s impact.
“Skin rash hernia images” are invaluable for understanding the broader impact of hernias on the integumentary system. Recognizing these skin changes is crucial, as some (like discoloration) demand immediate surgical attention, while others (like intertrigo or fungal infections) require specific dermatological management in conjunction with hernia care.
Hernia Treatment
The primary treatment for most symptomatic hernias, particularly those that are growing, causing pain, or posing a risk of complications, is surgical repair. While some small, asymptomatic hernias might be observed, and specific types like hiatal hernias can sometimes be managed non-surgically, definitive “hernia treatment” usually involves an operation to return the protruding tissue to its correct place and strengthen the weakened abdominal wall. The appearance of the surgical site and subsequent healing process are also crucial aspects to consider, especially for patients looking at “hernia treatment” outcomes.
Comprehensive aspects of hernia treatment include:
- Non-Surgical Management (Limited Application):
- Watchful Waiting: For very small, asymptomatic inguinal hernias in men, a “watch and wait” approach may be considered, particularly if surgical risks outweigh potential benefits. This involves regular monitoring for symptom progression. This is generally not recommended for femoral hernias due to higher rates of strangulation.
- Trusses or Binders: These supportive garments can temporarily help hold a reducible hernia in place and alleviate discomfort. However, they do not cure the hernia, can cause skin irritation or pressure sores if not fitted properly, and are not recommended as a long-term solution or for preventing complications like strangulation. Their use is typically reserved for patients unfit for surgery or awaiting surgery.
- Lifestyle Modifications (for Hiatal Hernias): For hiatal hernias, treatment often focuses on managing gastroesophageal reflux disease (GERD) symptoms. This includes dietary changes, elevating the head of the bed, avoiding large meals, weight management, and medications (e.g., antacids, proton pump inhibitors). Surgery is reserved for severe symptoms or complications.
- Surgical Repair (Herniorrhaphy/Hernioplasty):
- Open Hernia Repair:
- Procedure: Involves making a single, larger incision directly over the hernia site. The surgeon pushes the protruding tissue back into the abdomen.
- Mesh Placement (Hernioplasty): In most cases, a synthetic mesh is then sewn over or under the weakened area to reinforce the abdominal wall, significantly reducing recurrence rates.
- Tissue Repair (Herniorrhaphy): In some instances, especially for smaller hernias or specific patient profiles, the surgeon may simply stitch the weakened muscle and fascia back together without mesh.
- Recovery: Typically involves a longer recovery period compared to laparoscopic surgery, with more post-operative pain and a more visible scar.
- Scar Appearance: The resulting scar is usually a linear incision, varying in length depending on the hernia size and location. It typically starts red and raised, gradually fading and flattening over several months to a year, though it will remain visible.
- Laparoscopic Hernia Repair:
- Procedure: Performed using several small incisions (usually 3-4) through which a laparoscope (a thin, lighted tube with a camera) and surgical instruments are inserted. The surgeon views the procedure on a monitor.
- Mesh Placement: A mesh patch is almost always used in laparoscopic repairs and is secured from the inside of the abdominal wall.
- Types: Transabdominal Preperitoneal (TAPP) and Totally Extraperitoneal (TEP) are common approaches, differing in how the mesh is placed relative to the peritoneum.
- Recovery: Generally associated with less post-operative pain, a faster recovery, and a quicker return to normal activities due to smaller incisions.
- Scar Appearance: Consists of multiple small scars (typically 0.5-1.5 cm each) which are less noticeable than a single large incision. They also fade over time.
- Robotic Hernia Repair:
- Procedure: Similar to laparoscopic surgery, but the surgeon uses a robotic console to control instruments, offering enhanced dexterity, precision, and 3D visualization.
- Benefits: Can be particularly useful for complex or recurrent hernias, offering surgeons greater control.
- Recovery and Scars: Similar advantages to conventional laparoscopic surgery in terms of recovery time and scar aesthetics.
- Open Hernia Repair:
- Post-Operative Considerations and Skin Healing:
- Incision Care: Keeping the incision sites clean and dry is crucial to prevent infection. Patients are given instructions on dressing changes and signs of infection (e.g., increased redness, pus, fever).
- Swelling and Bruising: It is common to experience some localized swelling and bruising around the surgical site after hernia repair. This usually resolves within a few weeks.
- Numbness or Tingling: Nerve irritation or transection during surgery can lead to temporary or sometimes permanent areas of numbness or altered sensation around the incision.
- Seroma/Hematoma: Fluid (seroma) or blood (hematoma) collections can sometimes form under the skin near the surgical site, appearing as soft swellings. Most resolve on their own, but some may require drainage.
- Scar Maturation: Scars evolve over time. Initially, they may be red, raised, and firm. Over months, they typically flatten, soften, and lighten in color. Protecting scars from sun exposure can help minimize discoloration.
- Recurrence: While surgical techniques have improved, hernia recurrence is possible, especially in certain types of hernias or in patients with risk factors. A new bulge at or near the original site indicates recurrence.
- Specific Hernia Treatment Approaches:
- Umbilical Hernias: In infants, many close spontaneously. If persistent beyond age 4-5 or very large, surgical repair is performed. In adults, surgical repair is almost always recommended due to the risk of incarceration.
- Incisional Hernias: Often more complex to repair due to scar tissue and larger defects. Mesh is almost always used, and sometimes complex reconstructive techniques are required.
- Femoral Hernias: Due to a high risk of strangulation, femoral hernias are almost always recommended for surgical repair upon diagnosis.
Effective “hernia treatment” is individualized based on the hernia type, size, symptoms, the patient’s overall health, and surgeon’s expertise. While the focus is on repairing the underlying defect, understanding the visual aspects of post-operative healing and potential skin complications is also an integral part of comprehensive patient care.