When parents observe a distinct protrusion around their newborn’s belly button, understanding the characteristics of this presentation is crucial. This comprehensive guide details the various aspects of `Umbilical hernia in newborns symptoms pictures`, providing an in-depth look at what to expect and when to seek medical advice regarding these common infantile findings.
Umbilical hernia in newborns Symptoms Pictures
The primary symptom of an `umbilical hernia in newborns` is the visible and palpable protrusion or bulge that appears at or near the navel. This bulge is essentially a portion of the intestine or fatty tissue pushing through a weak spot in the abdominal muscles. The appearance of this bulge can vary significantly in size, shape, and consistency, and it often becomes more pronounced under specific circumstances. Understanding these nuances is key for parents observing their infant’s condition.
Typically, the `belly button bulge` associated with an umbilical hernia is:
- Soft and Reducible: In most cases, the hernia is soft to the touch and can be gently pushed back into the abdomen, a characteristic known as reducibility. This reduction might produce a gurgling sound as bowel contents return to the abdominal cavity.
- Variable in Size: The size of the hernia can range from very small, like a pea or a marble, to quite large, similar to a golf ball or even a small plum. The size does not necessarily correlate with the severity of the hernia, especially if it remains reducible.
- Round or Oval Shape: The protrusion usually has a smooth, rounded, or oval contour, originating directly from the umbilical area.
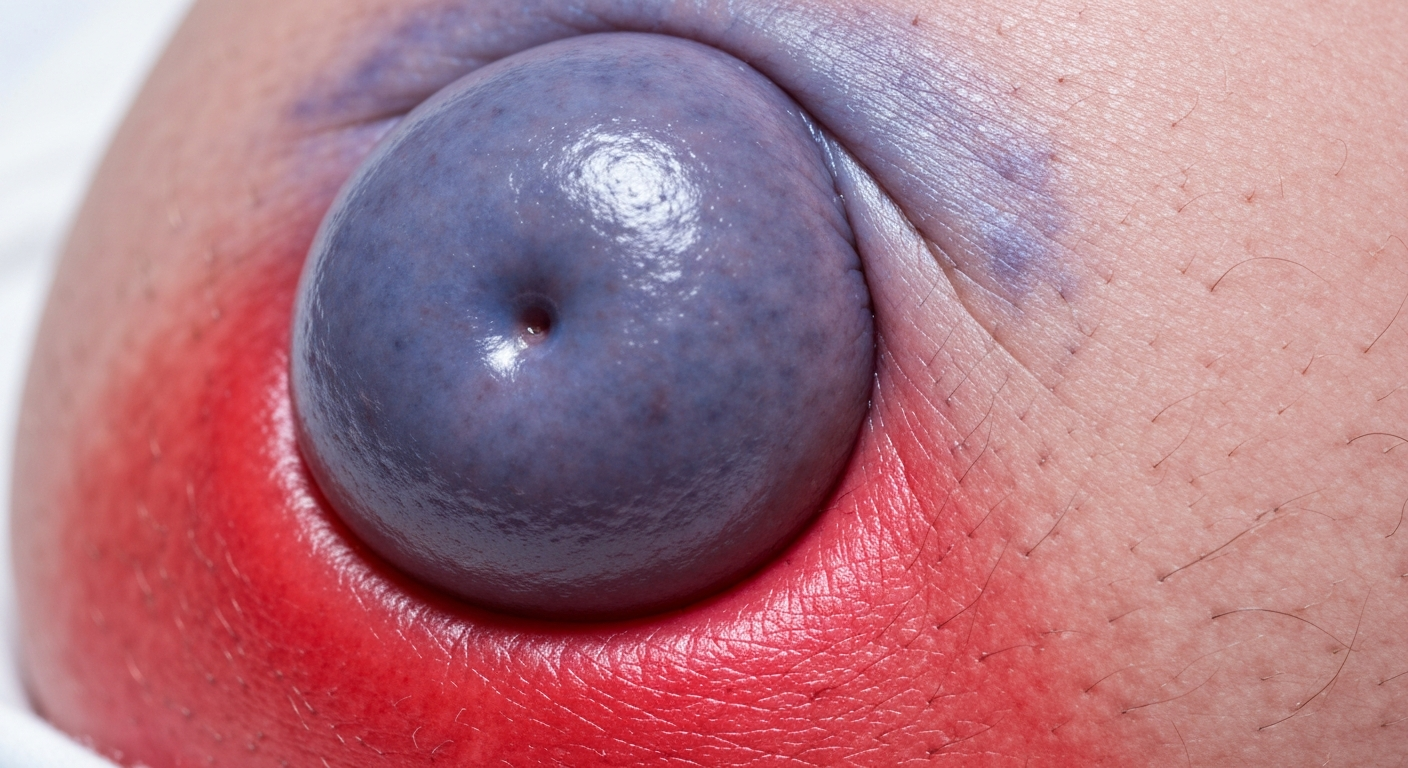
- Skin-Colored: The skin over the hernia generally retains its normal color, appearing no different from the surrounding abdominal skin. Any discoloration, such as redness, blueness, or purple hues, could indicate a complication and warrants immediate medical attention.
- More Prominent with Increased Abdominal Pressure: A hallmark symptom is the increased visibility and prominence of the bulge when the infant cries, strains during a bowel movement, coughs, or sits upright. When the baby is calm, relaxed, or lying down, the bulge might diminish significantly or disappear entirely. This dynamic change is a very strong indicator of an `umbilical hernia`.
- Absent or Minimally Visible at Rest: Many parents note that the hernia is barely perceptible or completely absent when their newborn is sleeping peacefully or is otherwise relaxed. The movement of the abdominal muscles during these relaxed states allows the internal contents to recede.
- Painless in Most Cases: For the vast majority of newborns, an `umbilical hernia` is not painful. Infants typically do not show signs of discomfort directly related to the hernia itself unless a complication arises. Fussiness or crying that makes the hernia more prominent is usually due to the underlying cause of the fussiness (hunger, gas, dirty diaper) rather than pain from the hernia.
Parents often describe feeling a soft, doughy sensation when palpating the bulge. The edges of the fascial defect (the hole in the abdominal wall) might be palpable as a firm ring around the base of the protrusion. This ring is the actual opening through which the hernia emerges.
Observing the hernia throughout the day can provide valuable information to the pediatrician. Noting how the hernia behaves during different activities, its maximum size, and whether it ever becomes firm or discolored are all important details for diagnosis and management planning. The visual confirmation of the bulge, especially when the infant is straining, is typically sufficient for a diagnosis of `newborn umbilical hernia`.
It’s important to differentiate between the appearance of an umbilical hernia and other conditions that might present as a lump in the navel area, such as an umbilical granuloma. An `umbilical granuloma` is a small, soft, moist, pink or red lump that forms after the umbilical cord detaches, resulting from an overgrowth of scar tissue. Unlike a hernia, a granuloma does not protrude more with straining and cannot be reduced into the abdomen.
Detailed observation of the `newborn’s belly button` over time can help confirm the nature of the bulge. Pediatricians often use a hands-on examination to assess the size of the fascial defect and the reducibility of the hernia, which are critical factors in determining the course of action.
Signs of Umbilical hernia in newborns Pictures
While the visible bulge is the most prominent symptom, there are specific `signs of umbilical hernia in newborns` that parents should be vigilant about. These signs can indicate the typical benign course of the hernia or, more rarely, suggest the development of a complication. Knowing these signs helps parents determine when to seek routine medical advice and when immediate attention is required.
Common and expected signs include:
- Dynamic Bulge: The hernia’s appearance changes with the infant’s activity level. It protrudes when crying, coughing, or straining, and flattens when the baby is relaxed. This dynamic nature is a reassuring sign that the hernia is freely reducible.
- Soft Texture: The hernia feels soft and easily compressible. This indicates that the contents are easily pushed back into the abdominal cavity.
- Normal Skin Color: The skin covering the hernia remains consistent with the color of the surrounding abdominal skin, without any redness, bruising, or bluish discoloration.
- Lack of Tenderness: The baby does not show signs of pain or discomfort when the hernia is gently touched or when it protrudes. There’s no wincing, guarding, or increased crying specifically linked to touching the hernia.
- Normal Feeding and Activity: The infant continues to feed well, sleep adequately, and display normal patterns of activity and alertness. The presence of the hernia does not typically interfere with these essential functions.
However, parents must be aware of `warning signs of umbilical hernia complications`, which necessitate immediate medical evaluation. These signs indicate that the hernia might have become incarcerated or, more severely, strangulated.
Critical warning signs include:
- Irreducible Hernia: The bulge becomes firm, hard, or tender and cannot be gently pushed back into the abdomen. This is a primary sign of `incarceration`, where the contents of the hernia sac (usually a loop of intestine) become trapped outside the abdominal cavity.
- Changes in Skin Color Over the Hernia:
- Redness: Intense redness of the skin over the hernia can indicate inflammation or a localized infection.
- Bluish or Purplish Discoloration: This is a very concerning sign, suggesting compromised blood supply to the incarcerated tissue. It is a strong indicator of `strangulation`, a medical emergency.
- Darker or Dusky Appearance: Any departure from normal skin tone, especially towards a darker hue, should prompt urgent medical consultation.
- Increased Pain and Fussiness: The infant cries inconsolably, especially when the hernia is touched. They may draw their legs up towards their abdomen or exhibit other signs of abdominal pain. This is a significant indicator that the hernia is causing discomfort or pain.
- Vomiting: Persistent vomiting, particularly green-tinged (bilious) vomit, can suggest an intestinal obstruction, which is a severe complication of an incarcerated hernia.
- Abdominal Swelling/Distension: The baby’s belly may appear generally swollen or distended, often accompanied by changes in bowel habits.
- Lack of Bowel Movements or Passing Gas: An incarcerated or strangulated hernia can block the passage of stool and gas, leading to constipation or absence of flatus.
- Lethargy or Decreased Activity: The infant appears unusually tired, less responsive, or has a noticeable decrease in their usual activity levels.
- Fever: While not a direct sign of the hernia itself, a fever in conjunction with other concerning signs can indicate infection or a more generalized illness associated with a complicated hernia.
- Firmness or Hardness of the Bulge: The hernia feels unyielding and rigid to the touch, unlike the usual soft texture. This rigidity, combined with irreducibility, is a red flag.
It is crucial for parents to understand that while most `newborn umbilical hernias` are benign and resolve spontaneously, vigilance for these concerning signs is paramount. If any of these warning signs are observed, especially irreducibility, skin discoloration, or signs of pain/distress, immediate medical attention is necessary. Early intervention in cases of incarceration or strangulation can prevent serious long-term complications, including damage to the bowel.
Documenting observations, even by taking discreet mental notes or written logs of changes in the hernia’s appearance or the infant’s behavior, can be helpful when communicating with healthcare providers. This careful monitoring contributes significantly to the optimal management of `umbilical hernia in infants`.
Early Umbilical hernia in newborns Photos
The presentation of an `early umbilical hernia in newborns` often starts subtly, evolving as the infant grows or as the abdominal muscles continue to develop. For many parents, the initial appearance can be a source of surprise or mild concern, prompting a visit to the pediatrician. Understanding what these early stages look like can help parents identify the condition sooner.
In many cases, an `umbilical hernia` is not immediately apparent at birth. While the umbilical ring is still somewhat open after the cord detaches, the hernia may only become noticeable a few weeks or even months after birth, typically between 1 and 3 months of age, when the umbilical stump has completely healed. The initial signs are often:
- Small, Pea-Sized Protrusion: The hernia might first appear as a very small, soft lump directly beneath the skin at the center of the navel, or slightly above or below where the umbilical cord once attached. It might be no larger than a pea or a small grape.
- Intermittent Appearance: At first, the bulge may only be visible intermittently. Parents might notice it momentarily when the baby is straining during a particularly vigorous cry or a hard cough, and then it quickly disappears when the baby calms down. This fleeting nature can sometimes make it difficult to catch during a routine doctor’s visit if the baby is relaxed.
- Slight Distention of the Navel: Instead of a distinct lump, some newborns may initially show a slight outward pouting or distention of the navel itself, which becomes more pronounced with abdominal pressure. The umbilicus may not fully retract inward as is typical for a fully healed navel.
- Softness and Easy Reducibility: Even in its earliest stages, the `early umbilical hernia` will almost always be soft to the touch and easily reducible. The ability to gently push the protrusion back into the abdomen is a key characteristic.
- Normal Skin Overlay: The skin covering the small protrusion will appear completely normal, matching the surrounding abdominal skin in color and texture. There are no signs of inflammation, discoloration, or thinning of the skin in the early phase.
Parents might first become aware of the `newborn belly button hernia onset` during diaper changes or bath time when they are closely observing their infant’s abdomen. The small size can make it easy to overlook if not specifically looking for it.
The development of an `umbilical hernia` is due to the failure of the abdominal muscles around the umbilical ring to close completely after birth. While this closure usually happens in the weeks and months following birth, if a small opening persists, it creates a weak spot. As the infant’s internal organs develop and the baby begins to cry and strain more frequently, the pressure can cause a small portion of bowel or fat to push through this opening, leading to the visible bulge.
It is very common for `early umbilical hernias` to gradually become more prominent in size over the first few months of life before they begin to shrink. This increase in size is often due to the growth of the infant and the increasing strength and frequency of abdominal muscle contractions (e.g., from more vigorous crying, laughing, or attempts to sit up). A hernia that was once pea-sized might expand to the size of a cherry or even a small plum.
Even with this initial growth, most `umbilical hernias in infants` remain benign and continue to be soft and reducible. The primary concern during these early stages is careful monitoring to ensure the hernia does not show signs of incarceration or strangulation. Pediatricians typically reassure parents that early, small, reducible hernias are expected to close on their own as the infant’s abdominal wall strengthens, usually by the time they are 1 to 5 years old. Regular check-ups allow the pediatrician to monitor the size of the defect and the hernia’s characteristics over time, ensuring that the `first signs of hernia` are being appropriately managed.
Skin rash Umbilical hernia in newborns Images
While an `umbilical hernia in newborns` itself is a muscular defect rather than a skin condition, various skin changes or `skin rashes near umbilical hernia` can sometimes be observed in the vicinity of the hernia. These are usually not part of the hernia’s direct presentation but can be secondary issues arising from irritation, infection, or, in rare severe cases, complications of the hernia itself. It is crucial to differentiate between general skin irritations common in newborns and specific skin manifestations that might signal a problem with the hernia.
Common skin concerns that might appear around the navel, unrelated to the hernia’s direct pathology, include:
- Diaper Rash or Irritation: If the hernia is large and extends into an area often covered by the diaper, skin irritation from moisture, urine, or feces can occur. This would present as redness, small bumps, or peeling skin, consistent with a typical diaper rash, but localized to the periumbilical region.
- Contact Dermatitis: Reaction to certain fabrics, detergents, lotions, or adhesive materials (if attempts were made to tape the hernia, which is strongly discouraged) can cause contact dermatitis. This appears as itchy, red, inflamed skin with potential blistering or dryness.
- Miliaria (Heat Rash): Small, red bumps or clear blisters can appear in skin folds or areas where heat and sweat are trapped, which could include the skin around a prominent hernia if clothing is tight or the baby is overdressed.
More specifically, `skin changes directly associated with the umbilical hernia` or its complications require careful attention:
- Localized Redness and Warmth: If the skin directly over the hernia becomes red and feels warm to the touch, this could indicate localized inflammation or an overlying skin infection. This may or may not be related to the hernia becoming incarcerated.
- Bluish or Purplish Discoloration: This is a grave sign. Any `umbilical hernia discoloration` towards blue or purple is a strong indicator of strangulation. Strangulation occurs when the blood supply to the herniated tissue (usually bowel) is cut off. This is a medical emergency requiring immediate surgical intervention to prevent tissue death and severe complications. The skin may also appear dusky or mottled.
- Intense Redness with Tenderness: A deep, angry red color that is very tender to the touch, potentially accompanied by swelling of the skin, could signal a severe inflammatory process or early strangulation.
- Thinning and Shininess of Skin: For very large umbilical hernias that have been present for an extended period, the overlying skin can become stretched, thin, and appear shiny due to the constant tension. While not usually painful, this can make the skin more fragile and susceptible to minor injury.
- Skin Breakdown or Ulceration: In extremely rare cases, if a very large hernia causes significant skin tension or if there’s prolonged irritation, the skin could break down, leading to an open sore or ulceration. This is a serious concern due to the risk of infection and potential exposure of underlying tissues.
- Pus or Drainage: If there is any discharge of pus, clear fluid, or foul odor from the navel area or from any break in the skin over the hernia, it indicates a bacterial infection. This requires prompt medical evaluation and treatment with antibiotics.
It is important for parents to avoid home remedies such as taping coins or other objects over the hernia, as these practices are ineffective in treating the hernia and can cause significant skin irritation, pressure sores, and even infection. Such practices can easily lead to a `belly button rash newborn` or more severe `umbilical skin infections`. Healthcare professionals explicitly advise against these methods.
When observing any `skin changes around the umbilical hernia`, it is vital to assess other accompanying symptoms in the newborn, such as fever, increased fussiness, changes in feeding, vomiting, or lethargy. The combination of skin discoloration (especially blue/purple), tenderness, and systemic symptoms is a definitive sign for an emergency room visit. For milder skin irritations, maintaining good hygiene and keeping the area clean and dry is important, but always consult with a pediatrician before applying any creams or treatments to the area, especially if a hernia is present.
Understanding the distinction between common newborn rashes and specific, concerning `umbilical hernia skin images` is critical for ensuring the infant receives appropriate and timely medical care.
Umbilical hernia in newborns Treatment
The `umbilical hernia in newborns treatment` approach is predominantly conservative, relying on observation due to the high rate of spontaneous closure. However, understanding the indications for surgical intervention and what to avoid is crucial for parents.
Conservative Management: Observation and Expectant Care
For the vast majority of `umbilical hernias in infants`, the primary treatment strategy is a “wait and see” approach. This is because the fascial defect, the opening in the abdominal wall, often closes naturally as the infant grows and the abdominal muscles strengthen. Key aspects of conservative management include:
- High Rate of Spontaneous Closure: Approximately 85-90% of umbilical hernias in newborns, especially those with smaller fascial defects (less than 1-2 cm in diameter), close on their own. This closure typically occurs by the time the child is 1 to 5 years old.
- Monitoring: Regular check-ups with a pediatrician are essential to monitor the hernia’s size, reducibility, and to watch for any signs of complications. The pediatrician will periodically assess the diameter of the fascial defect and the overall characteristics of the bulge.
- No Intervention Required: As long as the hernia remains soft, reducible, painless, and the overlying skin is normal, no specific intervention (like taping, binding, or special bandages) is needed or recommended.
- Parental Reassurance: A significant part of conservative management involves educating parents that these hernias are generally benign, do not cause pain, and are highly likely to resolve without surgery.
What NOT to Do
It is critical to emphasize what parents should absolutely avoid:
- Taping or Bandaging: Applying tape, coins, hernia belts, or any other objects over the hernia is a dangerous and ineffective practice. These methods do not help the hernia close and can lead to:
- Skin irritation, rashes, and blistering.
- Infections of the skin or navel.
- Pressure sores.
- In rare cases, they might even contribute to incarceration by pushing the bowel against the edges of the defect in a non-physiologic way.
- Aggressive Manipulation: Do not attempt to forcefully push the hernia back in. Gentle pressure, if needed for assessment by a professional, is one thing, but aggressive manipulation can cause injury.
Surgical Intervention: When is it Needed?
While most hernias resolve spontaneously, some require `umbilical hernia surgery infant` intervention. Indications for surgical repair typically include:
- Hernia Persisting Beyond a Certain Age: Most surgeons recommend repair if the hernia persists beyond 4-5 years of age. By this age, the likelihood of spontaneous closure significantly decreases.
- Large Hernia Defect: If the fascial defect is very large (e.g., greater than 2 cm in diameter) and shows no signs of shrinking, it may be less likely to close spontaneously, and surgery might be considered earlier, often by 2 years of age.
- Incarceration: This is a medical emergency. If the hernia becomes irreducible (cannot be pushed back in) and is associated with pain, tenderness, or discomfort, surgical repair is often necessary, sometimes urgently. Even if symptoms resolve with manual reduction by a doctor, surgery will often be recommended to prevent recurrence of incarceration.
- Strangulation: This is a surgical emergency. If the blood supply to the herniated tissue is compromised (evidenced by skin discoloration like blue or purple, severe pain, vomiting, or signs of bowel obstruction), immediate emergency surgery is required to prevent tissue necrosis.
- Very Large Hernias Causing Significant Skin Thinning: While rare, extremely large hernias might cause significant skin stretching and thinning, which could be a reason for earlier surgical consideration to prevent skin breakdown or rupture.
- Cosmetic Concerns: In some cases, a persistent, prominent hernia, even if benign, might be repaired before school age to address potential cosmetic concerns or social stigma.
The Surgical Procedure (Herniorrhaphy)
The surgical repair of an `umbilical hernia` (herniorrhaphy) in an infant is a common and generally safe procedure:
- Anesthesia: The surgery is performed under general anesthesia.
- Incision: A small incision is made either directly within the skin folds of the umbilicus or just below it, making the scar often virtually invisible once healed.
- Repair: The surgeon gently pushes the herniated contents back into the abdominal cavity. The small opening in the abdominal wall (the fascial defect) is then closed with sutures. In children, mesh is rarely used for umbilical hernia repair, unlike in adults, as the child’s own tissues are strong enough.
- Duration: The procedure typically takes less than an hour.
- Outpatient Procedure: Most children go home the same day.
Post-Operative Care
After `hernia surgery infant` repair:
- Pain Management: Mild pain relievers (like acetaminophen or ibuprofen, as advised by the pediatrician) can be given for discomfort.
- Wound Care: Parents will receive instructions on keeping the incision site clean and dry. Typically, the incision is covered with Steri-Strips or a waterproof dressing.
- Activity Restrictions: Generally, infants and young children can resume normal activities quickly. Strenuous activity or heavy lifting might be restricted for a short period, but for an infant, this usually means avoiding excessive straining.
- Follow-up: A follow-up appointment with the surgeon is usually scheduled within a few weeks to check on healing.
The prognosis after `umbilical hernia treatment newborn` surgery is excellent, with a very low recurrence rate. The key message for parents of newborns with an umbilical hernia is to remain calm, monitor for warning signs, and consistently consult with their pediatrician for guidance and reassurance. The natural history of spontaneous `umbilical hernia closure` is a comforting aspect for most families.