Recognizing subungual melanoma symptoms pictures is crucial for early detection and improved outcomes. This comprehensive guide details the various visual manifestations of this aggressive skin cancer under the nail, aiding in timely identification and fostering prompt medical evaluation for definitive diagnosis and treatment.
Subungual melanoma Symptoms Pictures
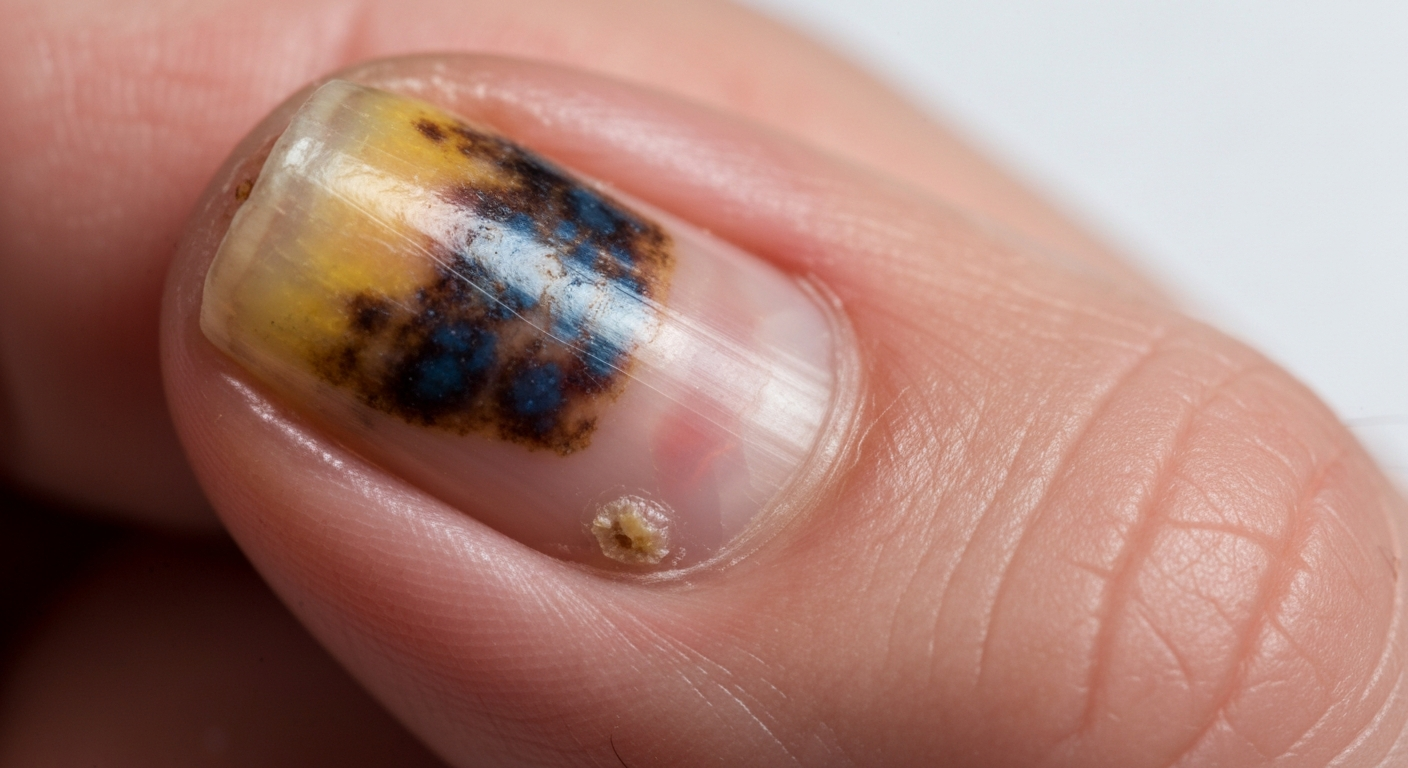
Subungual melanoma, a rare but aggressive form of melanoma, manifests primarily within the nail unit, leading to a variety of visual changes that can be captured in subungual melanoma symptoms pictures. The most common and frequently depicted symptom is longitudinal melanonychia (LMM), appearing as a brown or black streak extending from the nail matrix to the free edge of the nail plate. However, the characteristics of this streak, as well as other accompanying signs, are critical for differentiation from benign conditions.
The pigmentation observed in subungual melanoma is often highly variable. In symptom pictures, one might observe a range of colors from light brown to dark brown, black, blue-black, or even reddish-brown hues. This discoloration is typically uneven, with variations in intensity along the length and width of the band. Unlike benign racial melanonychia, which tends to be uniform in color and width, melanoma streaks frequently exhibit heterogeneity.
Key visual characteristics in subungual melanoma symptoms pictures often include:
- Irregular Pigmentation: The streak is not uniformly colored; it may have areas of darker and lighter shades within the same band. There might be dots, blotches, or streaks of different colors intermingled.
- Variable Width: The pigmented band typically varies in width, often widening proximally towards the cuticle or distally towards the free edge. This expansion can be subtle or pronounced and is a significant indicator. A width greater than 3 mm at its widest point is a common red flag.
- Blurred or Irregular Borders: The edges of the pigmented streak may appear fuzzy, notched, or poorly defined, rather than sharp and clear. This irregular border can indicate an invasive process.
- Rapid Change: A sudden onset or a noticeable change in an existing nail pigmentation—such as rapid widening, darkening, or alteration in color—is highly suspicious and warrants immediate investigation. This is often documented through sequential subungual melanoma pictures over time.
- Nail Dystrophy: The tumor growing beneath the nail plate can cause significant structural damage. Symptom pictures may show:
- Onycholysis: Separation of the nail plate from the nail bed, often leading to a whitish or yellowish discoloration under the nail.
- Nail Splitting or Cracking: The nail plate may split longitudinally (onychoschizia) or become brittle and prone to breakage.
- Thinning or Thickening of the Nail Plate: Irregular changes in nail thickness can occur.
- Ridging or Grooving: Vertical or horizontal lines on the nail surface may develop.
- Nail Plate Destruction: In advanced stages, the nail plate can be completely destroyed or lifted off, revealing an underlying ulcerated or tumorous mass.
- Ulceration or Bleeding: As the tumor grows, it can break through the nail bed, causing ulceration, spontaneous bleeding, or serosanguinous discharge. This may be seen as a dark, crusty area beneath or around the nail. These signs are often visible in more advanced subungual melanoma pictures and should prompt urgent medical attention.
- Nodule Formation: The development of a palpable or visible mass or nodule within the nail bed or under the nail plate is a concerning sign. This nodule can be pigmented or amelanotic (flesh-colored).
- Pain or Tenderness: While not always present, some patients experience pain, tenderness, or throbbing sensation in the affected digit, especially as the tumor grows and exerts pressure.
- Single Digit Involvement: Subungual melanoma typically affects only one digit, most commonly the thumb or the great toe. Involvement of multiple digits is rare and usually points to other conditions like racial melanonychia or drug-induced changes.
Careful examination of subungual melanoma symptoms pictures highlights the importance of observing not just the presence of pigmentation, but its specific characteristics, evolution, and associated changes in the nail unit and surrounding skin. Early recognition of these subtle yet significant visual cues is paramount for timely diagnosis and improved prognosis of this challenging nail cancer.
Signs of Subungual melanoma Pictures
Beyond the subjective symptoms, specific objective signs of subungual melanoma can be observed in diagnostic pictures, guiding clinicians towards a definitive diagnosis. These signs are often more specific and, when present, highly suggestive of malignancy. The most characteristic and widely discussed sign is Hutchinson’s sign, which represents the spread of pigment from the nail matrix into the periungual skin.
Detailed signs of subungual melanoma pictures commonly include:
- Hutchinson’s Sign: This is a critical indicator of subungual melanoma. It refers to the periungual discoloration, where the pigment from the nail matrix extends onto the adjacent skin of the nail folds (proximal and lateral) or the hyponychium (skin under the free edge of the nail). In pictures, this appears as a brownish or blackish stain on the cuticle or the skin immediately surrounding the nail.
- True Hutchinson’s Sign: Indicates invasive melanoma cells that have spread beyond the nail unit into the surrounding epidermal structures.
- Pseudo-Hutchinson’s Sign: This can occur in benign conditions, such as ethnic longitudinal melanonychia, where the cuticle is transparent, allowing visualization of underlying pigment from the nail matrix. However, in pseudo-Hutchinson’s sign, the pigment does not truly involve the skin. Differentiating between true and pseudo-Hutchinson’s sign often requires dermatoscopy or biopsy.
- Micro-Hutchinson’s Sign: A subtle form where the pigment spread is very fine and only visible under dermatoscopic examination.
- Nail Plate Destruction and Deformity: Progressive damage to the nail plate is a hallmark sign. Pictures show:
- Onychomycosis-like appearance: The nail may become thickened, discolored, and crumbly, mimicking a fungal infection, but unresponsive to antifungal treatments.
- Pterygium inversum unguis: Adherence of the distal nail bed to the ventral surface of the nail plate, causing a loss of the normal hyponychial space.
- Gross destruction: The entire nail plate may be lifted, absent, or show significant deformities like splitting or ridging. This exposes the underlying tumor.
- Presence of a Nodule or Tumor Mass: A visible or palpable lump, often pigmented but sometimes amelanotic (pink or red), within the nail bed or emerging from under the nail plate is a significant sign of subungual melanoma. These melanoma masses can be ulcerated or fungating in advanced stages.
- Ulceration and Crusting: Breakdown of the overlying skin or nail bed, resulting in open sores or crusts, particularly if accompanied by bleeding, points strongly towards malignancy. These lesions are often depicted in subungual melanoma images from later stages.
- Absence of Trauma History: While a history of trauma can sometimes trigger nail changes, a progressive, suspicious lesion without any preceding injury is a concerning sign for subungual melanoma.
- Lymphadenopathy: In more advanced cases, regional lymph node involvement (e.g., axillary nodes for finger lesions, inguinal nodes for toe lesions) can be a critical sign of metastasis. While not visible in subungual melanoma pictures of the nail itself, it is a crucial part of the clinical assessment.
- Single Digit Involvement in Adults: While children can have multiple benign pigmented nail streaks, a solitary pigmented band appearing in an adult, particularly on the thumb or great toe, significantly raises suspicion for subungual melanoma.
- Dermatoscopic Patterns: Although not a direct “picture” in the lay sense, dermatoscopic images reveal specific patterns indicative of subungual melanoma:
- Irregular longitudinal lines varying in color, thickness, and spacing.
- Micro-Hutchinson’s sign (pigment spread on the cuticle only visible under magnification).
- Presence of brown or black globules or dots.
- Triangular shape of pigmentation at the proximal nail matrix.
- Loss of parallelism of lines.
- Erosion or ulceration.
Recognizing these objective signs of subungual melanoma in pictures and during clinical examination is essential. Each sign, especially when combined, contributes to the clinical suspicion that necessitates biopsy for definitive diagnosis of nail unit melanoma.
Early Subungual melanoma Photos
Early subungual melanoma photos are vital for illustrating the subtle changes that often go unnoticed, leading to delayed diagnosis. The key to improving prognosis for subungual melanoma lies in identifying these initial, sometimes innocuous-looking, manifestations. While advanced disease can be striking, early signs are frequently mistaken for benign conditions like trauma, fungal infections, or racial pigmentation.
In early subungual melanoma photos, the presentation might be quite modest:
- Narrow, Lightly Pigmented Streak: Initially, the lesion may appear as a narrow (less than 3 mm wide), light brown or tan longitudinal band. It may not be intensely dark, making it easily dismissible. However, careful observation might reveal subtle irregularities not seen in benign streaks.
- Asymmetry and Irregularity: Even in its early stages, subungual melanoma often exhibits a degree of asymmetry in color or shape. The streak may be lighter on one side and darker on the other, or its width might not be uniform from the cuticle to the free edge. Early photos often capture these nuanced differences.
- Subtle Periungual Pigmentation: A very faint, barely perceptible brown discoloration on the cuticle or the nail fold (micro-Hutchinson’s sign) can be an early indicator. This subtle spread of pigment, though often missed with the naked eye, can be a crucial clue in early subungual melanoma photos when magnified or viewed with dermatoscopy.
- Change in an Existing Lesion: A pre-existing pigmented band that suddenly starts to darken, widen, or change its internal structure is highly suspicious. Tracking these changes with serial early subungual melanoma photos over months can be invaluable.
- Single Digit Involvement in a Non-Ethnic Individual: While common in darker skin types, a new solitary longitudinal melanonychia in a Caucasian individual, especially on the thumb or great toe, should always be viewed with suspicion.
- Lack of Response to Treatment for Benign Conditions: If a suspected fungal infection or hematoma under the nail does not resolve with appropriate treatment, or if the pigmentation persists and changes, melanoma should be considered.
The “ABCDE” rule, commonly used for cutaneous melanoma, has been adapted for subungual melanoma to aid in early detection. When examining early subungual melanoma photos, consider these criteria:
- A for Age and Ethnicity, and Amputation of digit in past:
- Age: Peak incidence in individuals aged 50-70 years, but can occur at any age.
- Ethnicity: Higher incidence in African Americans, Asians, and Native Americans, where it represents a higher proportion of all melanomas.
- Amputation of digit in past: If a digit has been previously amputated due to subungual melanoma, new or suspicious lesions on other digits should be evaluated carefully.
- B for Band (longitudinal band), Breadth (greater than 3mm), and Bleeding:
- Band Characteristics: A brown or black longitudinal band.
- Breadth: A band wider than 3 mm, especially if it’s changing in width or shape.
- Bleeding: Spontaneous bleeding or serosanguinous discharge from under the nail, or a history of bleeding without significant trauma.
- C for Change and Color:
- Change: Rapid increase in size or change in morphology of the pigmented band (darkening, widening, development of irregular borders).
- Color: Heterogeneity of color within the band (multiple shades of brown, black, blue-black), or areas of depigmentation (regression).
- D for Digit Most Commonly Involved and Dermatoscopy:
- Digit: Most frequently affects the thumb or the great toe, but any digit can be involved. Single digit involvement is more suspicious than multiple.
- Dermatoscopy: Reveals specific patterns: irregular brown or black dots or globules, homogeneous brown or black pigmentation, triangular shape at the proximal nail matrix, absence of parallel lines, and presence of micro-Hutchinson’s sign.
- E for Extension of Pigment and Evolution:
- Extension: Presence of Hutchinson’s sign, where pigment extends onto the periungual skin (cuticle, nail folds, or hyponychium).
- Evolution: Any discernible change or growth of the lesion over time, including new pain, tenderness, or nodule formation.
- Periungual Pigmentation (Hutchinson’s Sign): As discussed, this is the most direct “skin rash” manifestation, where melanin pigment visibly spreads from under the nail onto the surrounding skin of the nail folds or the hyponychium. In images, this appears as a brown, black, or variegated discoloration on the cuticle or lateral nail folds, mimicking a stain. This is not a true inflammatory rash, but rather a sign of tumor cells migrating into the epidermis.
- Erythema and Edema (Redness and Swelling): The skin surrounding the affected nail may become red and swollen, indicative of inflammation. This can be mistaken for paronychia (nail fold infection) or cellulitis. However, in subungual melanoma, this inflammation is typically persistent and may not respond to antibiotic treatment. In pictures, this might look like a persistent localized redness.
- Ulceration and Crusting of Periungual Skin: As the tumor grows and invades the surrounding skin, it can lead to breakdown of the epidermis, forming ulcers. These ulcers may bleed, ooze, and form crusts. Images might show open sores with irregular borders, often with a dark base, on the nail folds or fingertip/toetip. This can be misdiagnosed as a chronic wound or infection.
- Scaling or Hyperkeratosis: The skin around the nail may become thickened and scaly, mimicking conditions like chronic eczema, psoriasis, or squamous cell carcinoma. This hyperkeratotic reaction can be a response to the underlying tumor or direct invasion. Pictures may show dry, flaky, or rough skin texture adjacent to the nail.
- Nodule or Mass on Adjacent Skin: In advanced cases, the subungual melanoma can extend directly into the surrounding skin, forming a visible or palpable nodule or tumor mass. This mass can be pigmented or amelanotic (flesh-colored to reddish), firm, and potentially ulcerated. Images would show a distinct growth on the digit, separate from the nail plate, but clearly associated with the primary lesion.
- Satellite Lesions: In very advanced or aggressive cases, small, separate melanoma lesions (satellite lesions) may appear in the skin surrounding the primary tumor. These are typically small, pigmented papules or nodules. While rare, their presence in subungual melanoma images indicates advanced local spread.
- Absence of typical “rash” characteristics: Unlike a widespread skin rash, the changes associated with subungual melanoma are highly localized to the affected digit. They do not typically spread to other body areas in the pattern of allergic reactions or viral exanthems.
- Biopsy: A full-thickness excisional biopsy of the nail matrix and nail bed is the gold standard for diagnosis. Depending on the size and location, a punch biopsy or shave biopsy might be performed, but care is taken to obtain sufficient tissue depth for histopathological assessment. The biopsy must include the entire lesion and extend deep enough to allow for Breslow thickness measurement.
- Histopathology: Microscopic examination by an experienced dermatopathologist confirms the diagnosis and provides critical information such as Breslow thickness (depth of invasion), presence of ulceration, mitotic rate, and lymphovascular invasion.
- Staging Workup: For confirmed cases of subungual melanoma, especially with Breslow thickness >1.0 mm or ulceration, further staging tests are performed:
- Sentinel Lymph Node Biopsy (SLNB): Recommended for lesions >0.8 mm thick or those with ulceration to detect regional lymph node involvement, which significantly impacts prognosis and subsequent treatment decisions.
- Imaging Studies: PET-CT scans, CT scans of the chest/abdomen/pelvis, and MRI of the brain may be used to detect distant metastasis in advanced cases.
- Blood Tests: LDH (lactate dehydrogenase) levels are sometimes used as a prognostic indicator.
- Wide Local Excision (WLE):
- Involves removing the melanoma with a margin of healthy tissue around it. For subungual melanoma, this often means removing the entire nail unit (nail plate, nail bed, and nail matrix).
- The extent of excision depends on the Breslow thickness and location. For thin melanomas (<1.0 mm), a conservative excision might be attempted.
- Skin grafting may be required to cover the defect after excision.
- Amputation:
- For invasive subungual melanoma, especially those with significant Breslow thickness, ulceration, bone invasion (osteoinvasion), or recurrence, amputation of the affected digit (typically at the distal phalanx or higher) is often necessary to achieve clear margins and prevent local recurrence.
- This is a radical but often life-saving procedure, aiming for complete eradication of the cancer.
- The decision for amputation is carefully weighed against the functional and psychological impact on the patient.
More from my site:
By carefully scrutinizing early subungual melanoma photos against these criteria, healthcare professionals and educated patients can significantly improve the chances of identifying this aggressive nail cancer at a more curable stage.
Skin rash Subungual melanoma Images
While subungual melanoma primarily affects the nail unit, the term “skin rash” in the context of subungual melanoma images refers to changes in the skin immediately surrounding the nail (periungual skin), which can resemble or be mistaken for inflammatory skin conditions. These skin changes are usually indicative of either tumor extension or an inflammatory reaction to the underlying malignancy. It is crucial to distinguish these specific manifestations from common dermatological rashes.
Skin rash subungual melanoma images typically depict localized skin involvement rather than a widespread eruption. The key features to look for include:
The deceptive nature of these skin changes means that subungual melanoma is often misdiagnosed as chronic paronychia, pyogenic granuloma, fungal infection (onychomycosis), verruca (wart), or even benign trauma-induced hematoma. Therefore, any persistent or progressive periungual inflammation, ulceration, or pigmentation that does not respond to conventional therapies should raise suspicion for subungual melanoma and warrant biopsy. Skin rash subungual melanoma images serve as a critical educational tool to highlight these often-overlooked cutaneous manifestations, urging a high index of suspicion in clinical practice.
Subungual melanoma Treatment
Subungual melanoma treatment requires a comprehensive, multidisciplinary approach, tailored to the stage of the cancer, its location, and the patient’s overall health. Early diagnosis is paramount for effective treatment and improved prognosis. The cornerstone of subungual melanoma treatment is surgical excision, often complemented by various adjuvant and systemic therapies, particularly for advanced or metastatic disease.
Diagnosis and Staging for Subungual Melanoma
Before initiating treatment for subungual melanoma, accurate diagnosis and staging are crucial. This typically involves:
Surgical Treatment for Subungual Melanoma
Surgery remains the primary and most effective treatment for subungual melanoma. The goal is complete surgical removal of the tumor with clear margins while attempting to preserve as much function and cosmesis as possible.