Recognizing the visual cues of a life-threatening infection is paramount, and this article aims to provide an in-depth exploration of Sepsis symptoms pictures. Understanding these observable signs can be critical for prompt medical intervention, improving patient outcomes significantly in cases of suspected sepsis.
Sepsis Symptoms Pictures
When examining sepsis symptoms pictures, healthcare professionals and the public alike are looking for a constellation of systemic responses that indicate the body’s severe reaction to infection. These visual indicators are often a critical first step in identifying a patient who may be developing or already suffering from sepsis, severe sepsis, or septic shock. Early recognition from these pictures and clinical signs is crucial for effective sepsis management and improved prognosis.
The visual evidence in sepsis symptoms pictures can range widely, reflecting the diverse ways an infection can overwhelm the body. Patients might display general signs of acute illness, but specific markers often point directly to sepsis. These pictures often capture a patient in distress, exhibiting symptoms that demand immediate medical attention. It’s not just about the presence of a symptom, but often its severity and rapid onset. The visible impact on various organ systems becomes evident in advanced stages.
Key symptoms to look for in sepsis pictures include:
- Altered Mental State Pictures: Images might show confusion, disorientation, slurred speech, or unusual drowsiness. This can range from mild agitation to profound lethargy or unresponsiveness, critical indicators of brain dysfunction due to systemic inflammation and reduced cerebral perfusion.
- Rapid Breathing and Shortness of Breath Photos: Patients often exhibit tachypnea, or abnormally rapid breathing. Pictures may capture visibly labored breathing, use of accessory muscles, or gasping, indicating respiratory distress and the body’s attempt to compensate for metabolic acidosis or hypoxemia.
- Extremity Discoloration Images: Look for visual signs of poor circulation, such as bluish or pale discoloration of the fingers, toes, or lips (cyanosis). This is a strong indicator of inadequate oxygenation and perfusion to peripheral tissues, a hallmark of severe sepsis and septic shock.
- Skin Changes and Rashes: While a dedicated section will cover this, generalized paleness, mottling (patchy discoloration), or a clammy appearance are important sepsis skin signs.
- Fever or Hypothermia: While not directly visible in a still picture, the context accompanying sepsis symptoms pictures often references core body temperature. Extreme fever or, conversely, abnormally low body temperature (hypothermia) are common signs of systemic inflammatory response.
- Increased Heart Rate Pictures: While the rate itself isn’t visible, patients in photographs may appear agitated or distressed, reflecting a rapid pulse (tachycardia). This is the cardiovascular system working overtime to maintain organ perfusion.
- Reduced Urine Output: Although not directly observable in a picture of the patient, medical contexts related to sepsis images often highlight concerns about kidney function. Severely reduced urine production indicates acute kidney injury, a common complication of sepsis.
- Extreme Pain or Discomfort: Pictures might convey a patient in obvious pain, grimacing, or exhibiting guarding behavior, particularly if the original infection site is a source of severe pain. This pain can be diffuse or localized.
- Weakness and Fatigue: Images may show a patient appearing extremely weak, unable to sit up, or demonstrating profound muscle weakness. This generalized debility is a common feature of severe systemic illness.
- Sweating and Clammy Skin: Visuals might depict a patient with a visibly sweaty or clammy forehead and skin, often associated with a feeling of dread or impending doom, reflecting the body’s stress response.
These sepsis symptoms pictures serve as powerful educational tools, highlighting the urgent need for medical evaluation. Recognizing even a few of these signs together should trigger suspicion for sepsis and prompt immediate medical consultation for accurate diagnosis and aggressive sepsis treatment protocols. Early identification of these visual clues is critical for initiating timely interventions.
Signs of Sepsis Pictures
Delving deeper into signs of sepsis pictures, we often look for more objective and measurable physiological responses that are indicative of organ dysfunction. These are the clinical signs that healthcare providers meticulously observe, measure, and track when suspecting a patient has sepsis. The visual presentation of these signs in photographs can sometimes be subtle, requiring an understanding of the underlying physiological changes they represent. Accurate interpretation of these septic shock visible signs is crucial for rapid diagnosis and initiation of emergency sepsis care.
The progression from infection to sepsis involves a complex interplay of the immune system, and the physical signs of sepsis pictures often reflect this systemic breakdown. Unlike general symptoms which are subjective, signs are objective findings. For instance, while a patient might feel short of breath (symptom), rapid respiratory rate is a measurable sign. Visual aids highlighting these objective signs are invaluable for training and quick assessment in clinical settings. Understanding the body’s response to infection images helps in differentiating sepsis from other severe illnesses.
Specific observable signs of sepsis pictures include:
- Rapid or Shallow Breathing Photos: Visible chest wall movement can indicate tachypnea (respiratory rate > 20 breaths/minute) or bradypnea in severe cases. Pictures might capture the effort involved, flaring nostrils, or pursed-lip breathing.
- Tachycardia Images: While heart rate isn’t directly visual, pictures of patients exhibiting signs of distress, restlessness, or pale skin can indirectly suggest a rapid heart rate (> 90 beats/minute), as the body attempts to compensate for poor circulation.
- Hypotension (Low Blood Pressure) Manifestations: Although blood pressure itself isn’t visible, images might show extreme pallor, listlessness, or signs of shock (e.g., collapsed veins, very faint radial pulse if palpation were occurring). These are severe septic shock visible signs.
- Oliguria/Anuria (Reduced Urine Output): While not directly visible on the patient, photographs depicting medical equipment might show minimal urine in a catheter bag, or the patient’s general condition could suggest severe dehydration or kidney impairment.
- Altered Capillary Refill Time (CRT) Images: Pictures of hands or feet, especially fingers and toes, might show prolonged capillary refill time, where pressing on the nail bed and releasing shows a slow return of color, indicating poor peripheral perfusion. This is a critical septic shock assessment sign.
- Mottled Skin and Cyanosis: These are powerful signs of sepsis pictures. Mottling appears as a patchy, marbled pattern, especially on the extremities and trunk, due to microvascular disturbances. Cyanosis, a bluish discoloration, signifies profound hypoxemia.
- Petechiae and Purpura: These distinct skin lesions (small red/purple spots, larger bruises) are direct visual signs of coagulopathy and capillary leakage, often indicating severe sepsis or purpura fulminans, a critical subset of skin rash sepsis images.
- Edema and Swelling: Generalized or localized swelling (edema) can be present, particularly in the extremities or face, indicating fluid shifts and capillary leak, common in systemic inflammation.
- Jaundice (Yellow Skin/Eyes): Pictures might reveal a yellowish discoloration of the skin and sclera (whites of the eyes), indicating liver dysfunction, a potential complication of severe sepsis.
- Hypoxia (Low Oxygen Saturation): While directly measured with a pulse oximeter, patients in pictures with respiratory distress or cyanosis are often hypoxic.
- Changes in Body Temperature: As mentioned, fever (>38°C or 100.4°F) or hypothermia (<36°C or 96.8°F) are objective signs, though requiring a thermometer to confirm. The visual context might imply these temperature extremes.
Each of these signs of sepsis pictures contributes to a comprehensive clinical picture, allowing healthcare providers to rapidly assess the severity of the patient’s condition. Prompt recognition of these objective indicators is paramount for initiating life-saving sepsis treatment and management protocols, including aggressive fluid resuscitation and timely administration of antibiotics for sepsis.
Early Sepsis Photos
Identifying early sepsis photos can be exceptionally challenging, yet it is arguably the most critical aspect of improving survival rates. Early sepsis symptoms can be subtle and non-specific, often mimicking other common illnesses like the flu or a bad cold. This is why recognizing the initial sepsis signs and understanding their context is so vital. These photographs aim to capture the moments when the body first begins to show a significant, although not yet catastrophic, response to an infection. The goal is to highlight the subtle cues that differentiate a simple infection from one that is progressing towards a life-threatening septic event.
The progression from infection to early sepsis means that the body’s immune response is starting to become dysregulated. Early sepsis photos often depict individuals who are clearly unwell but may not yet show the dramatic organ dysfunction seen in severe sepsis or septic shock. The focus here is on vigilance and prompt action, as every hour of delay in appropriate sepsis treatment significantly increases mortality. Training with early warning signs of sepsis through visual aids can empower both medical professionals and caregivers to act swiftly.
Key indicators to look for in early sepsis photos include:
- Sudden Onset of Confusion or Disorientation: A person who was previously lucid but now seems confused, forgetful, or unusually quiet. This can be a very subtle but significant change in mental status. These onset of sepsis pictures are crucial for older adults.
- Unexplained Weakness or Malaise: An individual appearing profoundly tired, weak, or having difficulty performing routine tasks, beyond what would be expected for a common cold. This generalized feeling of being unwell is a frequent initial sepsis sign.
- Chills or Shivering with Fever: Pictures might convey a person shivering uncontrollably, even when bundled up, accompanied by a fever. This indicates the body’s intense thermoregulatory response to an infection.
- Rapid Heart Rate (Tachycardia) without Obvious Exertion: While not visually direct, a patient appearing restless or anxious might be experiencing an elevated heart rate, a physiological stress response.
- Fast Breathing (Tachypnea) Beyond Normal Exertion: Noticeably quicker breathing than usual, even at rest. This can be subtle and often overlooked in early sepsis photos.
- Generalized Feeling of Being Unwell or “Just Not Right”: This is a subjective symptom, but photos might show a patient with a worried or distressed expression, unable to articulate precisely what feels wrong.
- Warm, Flushed Skin (Early Vasodilation): In the initial stages, the skin might appear unusually warm to the touch and flushed due to vasodilation, a contrast to the pallor or mottling of later stages.
- Reduced Appetite or Nausea: While not specific, a sudden and severe loss of appetite or persistent nausea in someone with a suspected infection can be an early indicator of systemic illness.
- Pain or Discomfort at the Site of Infection: If there’s a visible wound or localized infection (e.g., cellulitis, abscess), images might show increasing redness, swelling, warmth, and tenderness around that area.
- Difficulty Waking Up or Staying Awake: A subtle but important sign, especially in children and the elderly, where lethargy goes beyond normal tiredness. These are critical pre-septic shock images for vulnerable populations.
- Decreased Urination: While not a visual symptom directly, if the patient is observed for extended periods, this can be a key early sign of kidney strain.
Training with these early sepsis photos is vital for healthcare staff in emergency departments, intensive care units, and even primary care settings. Recognizing these subtle shifts and escalating concern promptly is the cornerstone of effective sepsis protocols and significantly improves patient outcomes. The ability to identify these subtle signs of deterioration requires keen observation and a high index of suspicion for sepsis detection.
Skin rash Sepsis Images
The appearance of a skin rash in sepsis images is a critically important visual cue that often signals a severe and rapidly progressing condition, potentially indicating meningococcemia, purpura fulminans, or other severe forms of sepsis. These rashes are not just cosmetic; they represent underlying pathological processes, such as coagulopathy, disseminated intravascular coagulation (DIC), and direct microbial damage to blood vessels. Recognizing the specific characteristics of various septic rash photos can expedite diagnosis and initiation of specific, life-saving sepsis treatments.
While not all sepsis patients develop a rash, when one does appear, it demands immediate attention. The presence of certain types of rashes, especially hemorrhagic ones, can indicate a medical emergency requiring the highest level of vigilance. Learning to distinguish these severe skin manifestations from benign rashes is a key skill for all healthcare providers and crucial for anyone assessing skin rash sepsis images. These visual markers are often seen in severe cases, indicating significant systemic compromise.
Detailed descriptions of skin manifestations commonly seen in sepsis images:
- Petechiae Sepsis Pictures:
- Appearance: Small (1-2 mm), flat, round, red, or purple spots on the skin. They are caused by capillary bleeding into the skin and do not blanch (fade) when pressed.
- Location: Can appear anywhere but are often seen on the trunk, extremities, and mucous membranes.
- Significance: Indicate platelet dysfunction or capillary fragility, often an early sign of coagulopathy. A rapidly spreading petechial rash is highly concerning for meningococcemia or other severe bacterial sepsis.
- Urgency: Extremely high. Requires immediate medical evaluation for suspicion of critical illness.
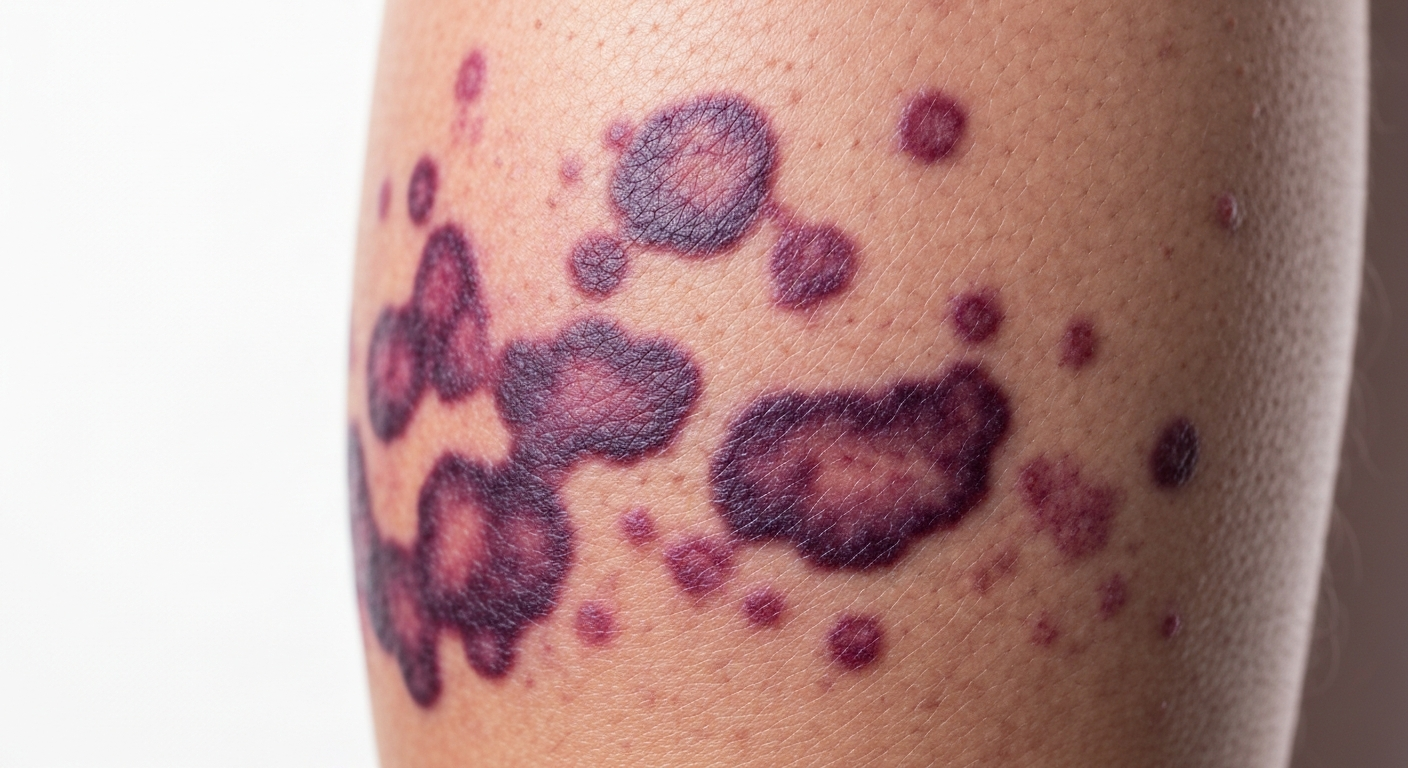
- Purpura Fulminans Images:
- Appearance: A severe and rapidly progressive skin lesion characterized by extensive, irregular, confluent areas of purpura (larger bruises) that progress to necrosis (tissue death). It often has a distinct violaceous (purplish-black) color.
- Location: Commonly affects the extremities (fingers, toes, nose, ears), but can spread to cover large body areas.
- Significance: A dramatic and rapidly evolving clinical syndrome of skin necrosis due to dermal vascular thrombosis and disseminated intravascular coagulation (DIC). It’s a severe complication of sepsis, particularly from meningococcal or streptococcal infections.
- Urgency: Critical. Represents a life-threatening medical emergency with high mortality rates, necessitating aggressive sepsis treatment protocols.
- Mottled Skin Sepsis:
- Appearance: A patchy, marbled, or reticulated (net-like) reddish-purple discoloration of the skin. It occurs due to vasodilation of venules and vasoconstriction of arterioles, leading to heterogeneous blood flow.
- Location: Most often observed on the extremities (knees, shins, arms) and trunk.
- Significance: Indicates poor peripheral perfusion and microcirculatory disturbances, a key sign of hypoperfusion and shock. It is an important indicator of severe sepsis and septic shock.
- Urgency: High. Indicates severe circulatory compromise and requires immediate intervention.
- Erythema in Sepsis:
- Appearance: Generalized redness of the skin. Can be diffuse or localized.
- Location: Can be widespread or concentrated around the source of infection (e.g., cellulitis).
- Significance: While common in many conditions, widespread erythema without blanching, especially if accompanied by fever and other sepsis symptoms, can indicate significant systemic inflammation. Localized erythema around a wound or infection site can point to the origin of sepsis.
- Urgency: Varies. If localized and contained, it might be an infection. If rapidly spreading or generalized with systemic symptoms, it warrants prompt investigation.
- Livedo Reticularis:
- Appearance: A persistent, net-like, reddish-blue discoloration of the skin, often more pronounced in cold temperatures but can be constant in sepsis. It’s similar to mottling but often more widespread and fine-meshed.
- Location: Primarily on the extremities and trunk.
- Significance: Signifies impaired microcirculation and blood flow, often associated with systemic inflammatory states and shock.
- Urgency: High. Suggests significant circulatory compromise, similar to mottling.
- Bullae or Vesicles (Blisters/Fluid-filled Lesions):
- Appearance: Fluid-filled blisters or pustules.
- Location: Can be localized or widespread.
- Significance: While less common in general sepsis, certain bacterial infections (e.g.,
Pseudomonas aeruginosa causing ecthyma gangrenosum, or severe streptococcal/staphylococcal infections) can cause necrotic bullae or rapidly progressive blistering. - Urgency: High. Suggests severe invasive infection and tissue damage.
- Jaundice:
- Appearance: Yellowish discoloration of the skin and the whites of the eyes (sclera).
- Location: Generalized.
- Significance: Indicates hyperbilirubinemia, often due to liver dysfunction, cholestasis, or hemolysis, all of which can be complications of severe sepsis.
- Urgency: High. Signals significant organ dysfunction, specifically hepatic involvement.
The rapid identification of these skin rash sepsis images, particularly petechiae and purpura, is critical for triggering immediate and aggressive sepsis emergency care. These skin signs often represent a critical turning point in the patient’s condition and demand swift medical action including diagnostic workup and targeted antibiotics for sepsis.
Sepsis Treatment
While the previous sections focused on the visual identification of symptoms and signs, understanding sepsis treatment is paramount, as prompt and aggressive intervention directly impacts patient survival. Seeing sepsis symptoms pictures must immediately lead to the initiation of evidence-based treatment protocols. Sepsis is a medical emergency requiring rapid diagnosis and immediate therapeutic measures, often referred to as a “sepsis bundle” or “sepsis resuscitation bundle.” The goal of sepsis management is to quickly halt the infection, support failing organs, and restore adequate perfusion.
The cornerstone of sepsis treatment protocols revolves around a time-sensitive approach, typically within the first few hours of recognition. Delays in administering broad-spectrum antibiotics for sepsis, for instance, significantly increase mortality. Modern sepsis guidelines emphasize a multidisciplinary approach involving critical care physicians, infectious disease specialists, and nurses to provide comprehensive care. The following outlines the key components of effective sepsis emergency care:
Immediate Interventions (Within 1-3 Hours of Sepsis Recognition):
- Fluid Resuscitation Sepsis:
- Action: Rapid intravenous (IV) administration of crystalloid fluids (e.g., normal saline, lactated Ringer’s solution) at a dose of 30 mL/kg for hypotension or a lactate level ≥ 2 mmol/L.
- Goal: Restore intravascular volume, improve blood pressure, and enhance organ perfusion.
- Monitoring: Closely monitor blood pressure, heart rate, urine output, and signs of fluid overload.
- Antibiotics for Sepsis:
- Action: Administration of broad-spectrum IV antibiotics within one hour of sepsis recognition (or suspicion).
- Rationale: To target the presumed infectious agent before definitive culture results are available. The choice of antibiotics is guided by local epidemiology, suspected source of infection, and patient factors.
- Goal: Eliminate the underlying infection as quickly as possible.
- De-escalation: Once culture results and sensitivities are known, antibiotics should be narrowed to target specific pathogens.
- Blood Cultures and Lactate Measurement:
- Action: Obtain at least two sets of blood cultures (aerobic and anaerobic) before administering antibiotics. Measure serum lactate levels.
- Rationale: To identify the causative pathogen for targeted therapy and to assess the degree of tissue hypoperfusion (lactate is a marker of anaerobic metabolism).
- Re-assessment: Re-measure lactate if initial levels are elevated to track resolution of hypoperfusion.
- Vasopressors Sepsis:
- Action: If hypotension persists despite adequate fluid resuscitation, vasopressors (e.g., norepinephrine, vasopressin) are initiated to maintain mean arterial pressure (MAP) ≥ 65 mmHg.
- Rationale: To constrict blood vessels and increase blood pressure, ensuring vital organ perfusion.
- Monitoring: Requires invasive hemodynamic monitoring (arterial line) and close titration in an intensive care setting.
Ongoing Management and Supportive Care:
- Source Control:
- Action: Identify and eliminate the source of infection as quickly as possible (e.g., drain an abscess, debride necrotic tissue, remove infected lines/devices, surgical intervention for perforated viscus).
- Rationale: Antibiotics alone may not be sufficient if a persistent source of infection remains.
- Respiratory Support:
- Action: Provide oxygen supplementation; intubation and mechanical ventilation may be required for acute respiratory failure (ARDS) or profound hypoxemia.
- Goal: Maintain adequate oxygenation and ventilation.
- Corticosteroids:
- Action: Low-dose IV corticosteroids (e.g., hydrocortisone) may be considered for patients in septic shock who are refractory to fluid and vasopressor therapy, particularly if they have adrenal insufficiency.
- Rationale: To modulate the inflammatory response and support blood pressure.
- Blood Product Transfusion:
- Action: Red blood cell transfusions may be given to maintain a hemoglobin target of 7-9 g/dL in stable patients. Platelets may be transfused for severe thrombocytopenia with bleeding.
- Rationale: To optimize oxygen-carrying capacity and coagulation.
- Glucose Control:
- Action: IV insulin infusion to maintain blood glucose levels between 140-180 mg/dL.
- Rationale: To prevent complications of hyperglycemia and hypoglycemia.
- Renal Replacement Therapy:
- Action: Dialysis or continuous renal replacement therapy (CRRT) may be initiated for acute kidney injury that is refractory to medical management.
- Rationale: To support kidney function and manage fluid, electrolyte, and acid-base imbalances.
- Nutrition:
- Action: Initiate enteral (preferred) or parenteral nutrition early in the course of critical illness once hemodynamically stable.
- Rationale: To prevent malnutrition and support immune function.
- Prophylaxis:
- Action: Stress ulcer prophylaxis (e.g., proton pump inhibitors) and venous thromboembolism (VTE) prophylaxis (e.g., low-molecular-weight heparin).
- Rationale: To prevent common complications in critically ill patients.
- Communication and Family Support:
- Action: Regular communication with patients and their families regarding prognosis and care decisions.
- Rationale: Essential for patient-centered care and shared decision-making.
Effective sepsis treatment requires continuous monitoring of vital signs, organ function (respiratory, cardiovascular, renal, neurological), and laboratory parameters. Any deterioration in a patient’s condition, even after initial stabilization, must trigger a re-evaluation of the treatment plan. The lessons learned from analyzing sepsis symptoms pictures and understanding the urgency they convey are directly translated into these aggressive and timely therapeutic interventions, emphasizing that every minute counts in the fight against sepsis.