Visual aids are invaluable for recognizing various dermatological conditions, and understanding the presentation of Erythema annulare symptoms pictures can significantly aid in identification. These images often depict the characteristic ring-shaped lesions, offering clear insights into this distinctive skin manifestation. Familiarizing oneself with these visual cues is crucial for accurate assessment of Erythema annulare symptoms pictures.
Erythema annulare Symptoms Pictures
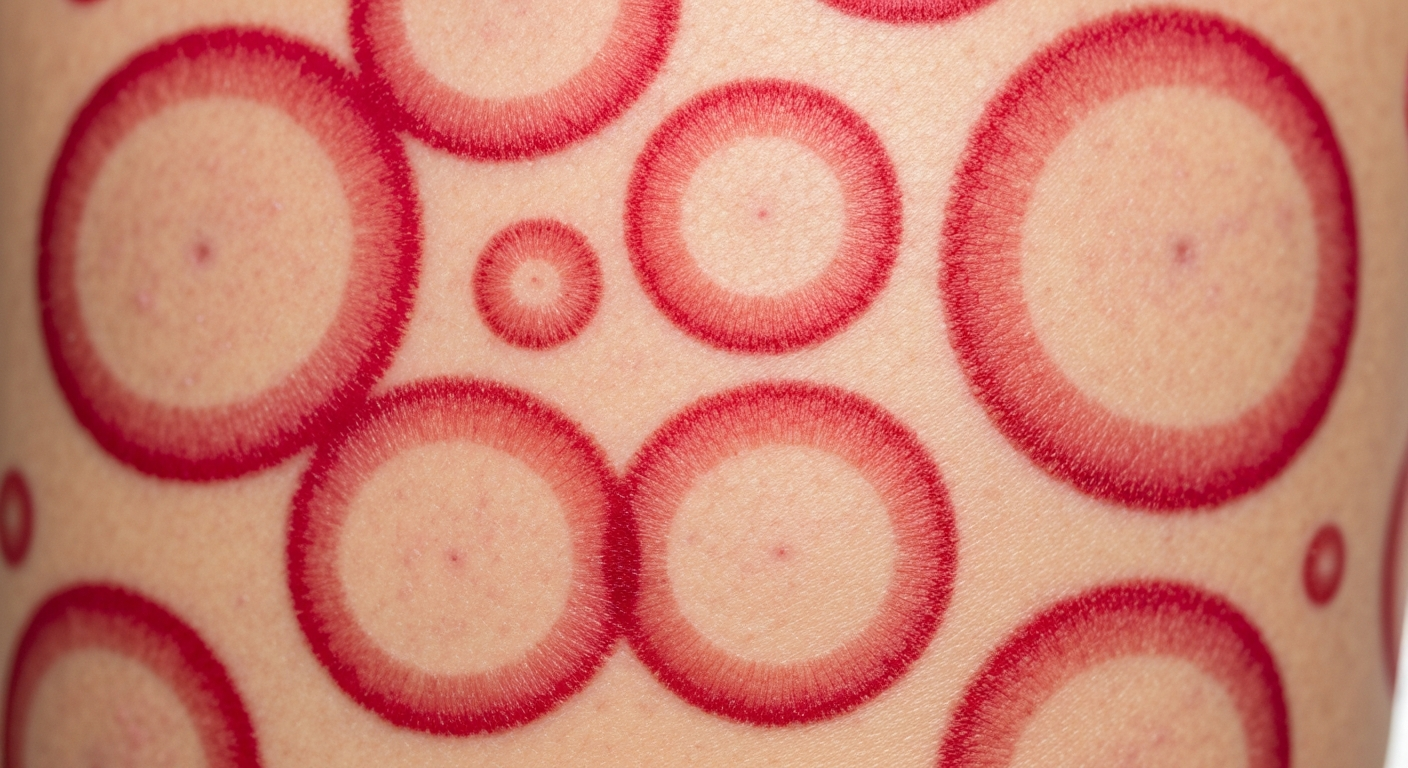
When examining Erythema annulare symptoms pictures, the most striking and consistent feature observed is the presence of distinctive, often widespread, annular or ring-shaped lesions. These lesions are typically erythematous, meaning they exhibit a red or reddish-pink coloration, which can vary in intensity from a subtle blush to a vivid crimson. The rings characteristically possess an outwardly expanding, raised, and firm border, which is often more intensely erythematous and palpable compared to the central area. This advancing edge represents the active inflammatory margin of the lesion. Within the confines of this ring, the skin often appears normal or slightly hyperpigmented, a phenomenon referred to as “central clearing.” This contrast between the inflamed periphery and the clearer center is a hallmark diagnostic feature visible in most Erythema annulare symptoms pictures. The texture of the raised border is usually smooth, though it can occasionally exhibit a very fine, almost imperceptible scale, particularly at its leading edge. Individual lesions can vary significantly in diameter, ranging from a few millimeters to several centimeters, and in some instances, multiple rings may coalesce or overlap, creating polycyclic, arcuate, or serpiginous patterns. These complex configurations, readily apparent in many Erythema annulare symptoms pictures, arise from the merging of adjacent or expanding rings, forming irregular and often visually captivating designs on the skin surface. The distribution of these lesions is often widespread, frequently affecting the trunk, extremities, and occasionally the face or neck. The presence of these highly characteristic, migrating annular lesions is a primary indicator for suspicion of Erythema annulare, making detailed observation of Erythema annulare symptoms pictures an essential step in understanding its clinical presentation. Careful analysis of the borders, the degree of central clearing, and the overall morphology provides invaluable insights into the nature of this dermatological condition. The dynamic nature of these lesions, where the rings slowly enlarge centrifugally, is a key characteristic that differentiates it from other annular dermatoses. The uniformity of the ring’s width, typically a few millimeters, further aids in identification across various Erythema annulare symptoms pictures. Occasionally, a lesion might exhibit a less pronounced central clearing, appearing as a more solid, yet still annular, patch of erythema, but this is less common than the classic appearance. The depth of erythema can also be influenced by factors such as skin phototype and the degree of inflammation present, contributing to variations seen in Erythema annulare symptoms pictures. These visual characteristics are fundamental in understanding the typical presentation and progression of Erythema annulare.
- Primary Lesion Morphology:
- Annular Rings: Distinctive, well-demarcated ring-shaped lesions.
- Erythematous Coloration: Red to reddish-pink hues, often brighter at the active border.
- Raised Border: Palpable, slightly elevated, and often firmer than surrounding skin.
- Active Margins: The leading edge of the ring shows the most intense inflammation and outward expansion.
- Central Clearing: The inner portion of the ring typically appears normal or minimally affected, contrasting with the inflamed border.
- Variable Size: Lesions can range from small rings (1-2 cm) to large, expansive patches (over 10 cm).
- Pattern Variations:
- Polycyclic Patterns: Formed by the confluence or intersection of multiple rings, creating scalloped or wavy edges.
- Arcuate Lesions: Incomplete rings or crescent-shaped configurations.
- Serpiginous Forms: Snake-like or winding patterns, often resulting from the migration of the annular lesions.
- Confluent Patches: Multiple lesions merging to create larger, irregularly shaped areas of erythema with partial clearing.
- Skin Texture and Surface Changes:
- Smooth Surface: Most commonly, the lesions have a smooth, non-scaly surface.
- Fine Scale: Occasionally, very fine, barely visible scaling may be present along the active border.
- Absence of Vesicles/Bullae: Typically, Erythema annulare does not involve blistering or fluid-filled lesions, which helps differentiate it from other annular dermatoses.
- Common Body Locations:
- Trunk: Back, chest, abdomen are frequently affected.
- Extremities: Arms, legs, thighs, and buttocks.
- Neck and Shoulders: Often observed spreading across these areas.
- Less Common Sites: Face, palms, and soles are less frequently involved but can occur.
- Dynamic Nature:
- Centrifugal Expansion: The rings typically enlarge slowly over days to weeks.
- Migratory Character: Lesions may appear, fade in one area, and then reappear in another, or expand continuously.
- Recurrence: Individual lesions or new lesions can recur over time, sometimes in the same or adjacent areas.
Signs of Erythema annulare Pictures
The characteristic signs evident in Erythema annulare pictures extend beyond mere morphology, encompassing the overall behavior and associated features of the skin condition. A key visual sign is the dynamic and often migratory nature of the lesions; they do not remain static but tend to expand outwards, with the active inflammatory border slowly advancing over days or weeks. This centrifugal spread, where the lesion grows from its center, is a defining characteristic. In many Erythema annulare pictures, one can discern the subtle yet distinct color gradient, with the most intense redness concentrated at the outer rim, gradually fading towards the center. This differential erythema signifies the active inflammatory process localized to the periphery. Furthermore, the palpability of the raised border is another crucial sign, even if not directly visible in a two-dimensional image; the firm texture of the margin is a clinical finding that complements the visual assessment. While primarily an asymptomatic condition, a subset of patients may experience mild pruritus (itching) associated with the lesions, particularly at the active borders. Although the itch is usually not severe, its presence can sometimes lead to excoriations if scratched, which might subtly alter the appearance in some Erythema annulare pictures. The absence of significant scaling or crusting is another important negative sign, distinguishing Erythema annulare from conditions like tinea corporis, which often present with prominent scaling. The lesions typically resolve without leaving behind any scarring, though post-inflammatory hyperpigmentation (darkening of the skin) can occur, especially in individuals with darker skin tones, and this residual discoloration may be visible in older Erythema annulare pictures of resolving lesions. The transient nature of individual rings, which can last for weeks or months before fading, only to be replaced by new ones elsewhere, also contributes to the overall clinical picture. This pattern of appearance and disappearance over time is a significant diagnostic clue. The lesions are usually flat or slightly elevated, generally lacking significant induration or nodularity, which helps differentiate them from deeper skin processes. Close examination of Erythema annulare pictures often reveals the consistency in the width of the erythematous border across different lesions within the same individual, highlighting the uniformity of the inflammatory response. Moreover, the lack of systemic symptoms in the majority of cases is a crucial differentiator; the rash is typically the sole manifestation, reinforcing its benign cutaneous nature. The distinct clarity of the central area, often returning to normal skin color and texture, stands in stark contrast to the persistent inflammation at the leading edge, providing a clear visual boundary for diagnostic evaluation. In instances where multiple lesions are present, their interaction can produce complex patterns, such as targetoid lesions (resembling a bullseye, though less common than classic rings) or interwoven configurations, each reflecting the underlying inflammatory process. The presence of these evolving and characteristic patterns is a key to identifying Erythema annulare. The progression from a small, erythematous macule or papule to a full-fledged annular lesion is another sign that can be inferred by comparing Erythema annulare pictures taken at different time points.
- Observable Clinical Signs in Erythema annulare Pictures:
- Centrifugal Expansion: Clear evidence of outward growth from a central point in progressive images.
- Defined Border: A sharply demarcated, often palpable, erythematous edge.
- Central Clearing: A distinct area of normal or hypopigmented skin within the ring.
- Color Gradient: More intense redness at the periphery, fading towards the center.
- Absence of Blistering: No vesicles or bullae typically present, distinguishing it from vesiculobullous annular conditions.
- Lack of Significant Scaling: Minimal to no prominent desquamation or peeling within the ring or at the border.
- Non-Scarring Resolution: Lesions typically fade without leaving permanent skin damage.
- Associated Symptoms (May influence appearance):
- Mild Pruritus: Occasional itching, predominantly at the active border, potentially leading to subtle excoriations.
- Asymptomatic Nature: Frequently, the rash presents without any subjective symptoms, emphasizing its visual diagnosis.
- Pattern and Distribution Clues:
- Multiple Lesions: Often, several rings are present simultaneously across various body sites.
- Symmetry: While not strictly symmetrical, lesions can appear on corresponding areas of the body.
- Migration and Resolution: Individual lesions may disappear from one area as new ones emerge elsewhere, or fade completely over time.
- Evolutionary Traits:
- Slow Progression: The enlargement of rings occurs gradually over days to weeks.
- Persistence: Individual lesions can persist for weeks to months before resolving spontaneously.
- Recurrence Potential: New outbreaks of rings are common, even after resolution of previous ones.
- Differential Diagnostic Features (by exclusion from visual cues):
- No Pustules: Absence of pus-filled lesions, differentiating from some infectious annular rashes.
- No Deep Induration: The lesions are generally superficial, lacking significant depth or firmness beyond the border.
- Absence of Prominent Systemic Signs: The skin rash is typically the isolated finding, without fever, malaise, or joint pain, although underlying conditions can be associated.
Early Erythema annulare Photos
Examining early Erythema annulare photos is crucial for understanding the initial presentation and subsequent evolution of this characteristic skin condition. In its nascent stages, Erythema annulare typically manifests as a small, erythematous macule or papule, usually no more than a few millimeters in diameter. These initial lesions are often indistinct and might easily be overlooked or mistaken for a common insect bite or a minor skin irritation. However, close observation in early Erythema annulare photos reveals that these small, reddish spots are the precursors to the distinctive annular rings. Over a period of several days to a week, this initial macule or papule begins to slowly enlarge, and a subtle but definite central clearing starts to emerge. Concurrently, the peripheral edge of the lesion becomes more elevated and distinctly erythematous, gradually forming the active, expanding border that defines the condition. The transition from a simple red spot to a nascent ring is a critical phase captured in early Erythema annulare photos. At this stage, the ring may be incomplete or arcuate, forming a crescent shape before fully enclosing into a circular configuration. The redness might not yet be as vivid or as sharply demarcated as in fully developed lesions, appearing as a softer, pinkish erythema. The palpability of the border, while present, may also be less pronounced in these early stages. The expansion is usually steady and uniform, indicating a continuous outward migration of inflammatory cells. Early Erythema annulare photos often highlight the isolated nature of these initial lesions before multiple rings potentially appear. The skin surrounding these early formations typically appears normal, without any widespread inflammation or additional associated dermatological features. It’s during this developmental phase that an accurate diagnosis can be most challenging, as the classic annular morphology may not yet be fully established. However, the consistent pattern of a reddish spot evolving into an expanding ring with central clearing, even if subtle, provides key diagnostic clues when analyzing early Erythema annulare photos. The absence of vesicles, pustules, or significant scaling in these initial stages further helps in narrowing down the differential diagnosis. Understanding these early visual cues is vital for timely identification and appropriate clinical management, especially for healthcare providers who frequently review dermatological images. The focus in early Erythema annulare photos should be on the incipient stages of ring formation, the subtle changes in skin texture, and the gradual development of the hallmark central clearing. This early recognition can often prevent unnecessary anxiety and lead to a more focused investigation for potential underlying associations. The uniform inflammatory process at the expanding edge, even in its early, less prominent form, is a consistent feature across various early Erythema annulare photos. The skin texture, though perhaps subtly elevated at the border, remains generally smooth and non-indurated, setting it apart from nodular lesions. The subtle pinkish hue of the developing ring in fairer skin types, or a faint brownish tint in darker skin types, also serves as an important visual descriptor in early Erythema annulare photos.
- Initial Presentation:
- Small Macule/Papule: Begins as a tiny, erythematous (red) flat spot or slightly raised bump.
- Indistinct Edges: Borders are often ill-defined in the earliest stages.
- Subtle Coloration: Initial redness may be a faint pink rather than a vivid red.
- Early Evolution (Days to Week):
- Gradual Enlargement: The initial spot slowly expands centrifugally.
- Emerging Central Clearing: A subtle pallor or return to normal skin color begins to appear in the center.
- Developing Border: The peripheral edge becomes more elevated and distinctly red, starting to form a ring.
- Arcuate/Incomplete Rings: Lesions may initially form crescent shapes before completing a full circle.
- Key Visual Cues in Early Photos:
- Absence of Prominent Scale: Usually smooth surface, minimal to no flaking.
- No Vesicles/Pustules: Lack of fluid-filled or pus-filled lesions.
- Localized Erythema: Redness concentrated to the developing lesion, surrounding skin is normal.
- Consistent Expansion: Evidence of the lesion growing outwards.
- Differential Features in Early Stages:
- Distinction from Insect Bites: Erythema annulare typically lacks a central punctum (bite mark) and progresses differently.
- Distinction from Urticaria: While raised and erythematous, Erythema annulare lesions are more persistent than transient hives and expand centrifugally, rather than appearing and disappearing rapidly.
- Distinction from Early Tinea: Tinea often presents with more pronounced scaling and sometimes pustules at the border, which are typically absent in early Erythema annulare.
- Importance of Early Recognition:
- Accurate Diagnosis: Helps confirm Erythema annulare and rule out other conditions.
- Monitoring Progression: Allows for observation of the characteristic growth pattern.
- Consideration of Underlying Causes: Early identification can prompt investigation for associated systemic conditions if clinically indicated.
Skin rash Erythema annulare Images
Analyzing skin rash Erythema annulare images provides a comprehensive overview of how this dermatological condition manifests across diverse body areas and in varying degrees of severity. These images consistently reveal the hallmark annular lesions, but the sheer number, size, and confluence of these rings can vary dramatically, creating a wide spectrum of visual presentations. In some skin rash Erythema annulare images, only a few isolated, perfectly formed rings might be present, scattered across the trunk or extremities. Each ring would display the classic features: a raised, erythematous border and a centrally cleared area, perhaps 2-5 cm in diameter. However, other images might depict a much more widespread eruption, with numerous lesions of different sizes appearing simultaneously. These may include smaller, developing rings alongside larger, well-established ones, painting a dynamic picture of the rash’s activity. The patterns can become quite complex in skin rash Erythema annulare images where multiple lesions coalesce. Instead of distinct circles, one might observe intricate polycyclic configurations, where several rings merge to form a scalloped or wavy border, creating large, irregular patches of erythema with partial central clearing. Serpiginous (snake-like) patterns are also common, resulting from the continuous expansion and merging of arcuate lesions. The overall distribution is often symmetrical, affecting both sides of the body, particularly the flanks, abdomen, chest, and proximal limbs. However, asymmetrical presentations are also possible, depending on the trigger or individual predisposition. Skin rash Erythema annulare images are invaluable in demonstrating how the rash typically spares certain areas, such as the palms, soles, and mucous membranes, which helps differentiate it from other generalized erythematous eruptions. The degree of erythema can also vary, influenced by factors like the individual’s skin tone, the duration of the lesion, and any minor trauma or irritation. In lighter skin tones, the redness is usually pronounced, while in darker skin tones, the active border might appear as a darker reddish-brown or violaceous hue. Post-inflammatory hyperpigmentation, a common sequela, can also be observed in resolving lesions in many skin rash Erythema annulare images, appearing as faint brownish marks where previous rings had been. The skin between the active lesions generally appears normal, without generalized inflammation or scaling, underscoring the localized nature of the eruption. The chronic and recurrent nature of the rash is also implied in many skin rash Erythema annulare images, with lesions appearing in various stages of development and resolution. This visual variability, from simple rings to complex, interwoven patterns, is a critical aspect of understanding the dermatological footprint of Erythema annulare, making a comprehensive review of skin rash Erythema annulare images essential for diagnostic and educational purposes. The persistent yet often self-limiting course of individual lesions, alongside the potential for new ones to emerge, means that a collection of skin rash Erythema annulare images over time would show a constantly evolving dermatological landscape. The absence of systemic signs such as fever or malaise, when considering the clinical context of these images, further reinforces the typically benign cutaneous presentation of this condition. The distinct “clear center, active border” principle remains consistent across nearly all skin rash Erythema annulare images, regardless of the complexity of the patterns formed. The uniform width of the active erythematous rim is another subtle but consistent feature often detectable.
- Overall Distribution Patterns:
- Trunk Dominance: Frequently and extensively affects the back, chest, and abdomen.
- Limb Involvement: Common on upper and lower extremities, including arms, thighs, and buttocks.
- Sparing of Acral Areas: Palms, soles, and mucous membranes are typically unaffected.
- Facial Involvement: Less common but can occur, especially in more generalized or persistent cases.
- Lesion Density and Extent:
- Sparse Eruption: A few isolated rings, well-spaced from each other.
- Moderate Eruption: Multiple rings of varying sizes scattered across several body regions.
- Widespread/Generalized Eruption: Numerous lesions covering large surface areas, potentially with extensive confluence.
- Complex Configurations (Formed by Coalescence):
- Annulus Mirabilis: Latin for “wonderful ring,” referring to the perfectly formed, often large, individual rings.
- Arcuate: Curved or crescent-shaped lesions.
- Serpiginous: Wavy or snake-like patterns, indicating migratory expansion.
- Polycyclic: Intersecting or merging rings creating intricate, multi-lobed designs.
- Gyrate: Convoluted, circling patterns.
- Targetoid (Rare): Concentric rings resembling a “bull’s-eye,” less typical for classic Erythema annulare but can occasionally be seen in variants or overlapping conditions.
- Appearance in Different Skin Tones:
- Lighter Skin: Bright red to pinkish-red lesions with distinct contrast.
- Darker Skin: Can present as dusky red, violaceous, or hyperpigmented reddish-brown lesions.
- Post-inflammatory Hyperpigmentation: More prominent and persistent in darker skin tones after resolution.
- Evolutionary Stages Depicted:
- Concurrent Lesions: Images often show lesions in different stages of development – early papules, expanding rings, and fading residual marks.
- Chronic Recurrence: The overall appearance may suggest a history of recurring outbreaks.
- Benign Nature: The overall appearance typically suggests a non-aggressive, superficial inflammatory process without deep tissue destruction.
Erythema annulare Treatment
While Erythema annulare is often a self-limiting condition that may resolve spontaneously over months to years, treatment is primarily focused on alleviating symptoms and managing the appearance of the rash, especially when it causes significant cosmetic concern or pruritus. It’s crucial to understand that treatment strategies for Erythema annulare are largely symptomatic and supportive, as there is no specific cure, particularly for idiopathic cases. The cornerstone of Erythema annulare treatment involves topical therapies aimed at reducing inflammation and erythema. Mild to moderate potency topical corticosteroids are frequently prescribed. These anti-inflammatory agents work by suppressing the immune response in the skin, thereby reducing the redness, swelling, and itchiness associated with the active borders of the lesions. Application is usually once or twice daily for a limited duration to minimize potential side effects such as skin atrophy. For more extensive or recalcitrant lesions, higher potency topical corticosteroids may be considered, always under strict medical supervision due to the increased risk of side effects. Calcineurin inhibitors, such as tacrolimus ointment or pimecrolimus cream, offer another topical option, particularly for sensitive areas where corticosteroid use is less desirable, like the face or skin folds. These agents modulate the immune response without the corticosteroid-associated risks of skin thinning. For patients experiencing pruritus, oral antihistamines can be highly effective. Non-sedating antihistamines are preferred for daytime use, while sedating antihistamines might be beneficial at night to aid sleep disrupted by itching. These medications help to counteract the histamine release that contributes to the sensation of itch. In cases where an underlying condition is identified or strongly suspected (e.g., infections, autoimmune diseases, certain malignancies), the most effective “treatment” for Erythema annulare involves addressing and resolving that primary etiology. For instance, if a specific infection is a trigger, treating the infection may lead to the resolution of the skin rash. However, it is important to note that a clear underlying cause is not always found. For severe, widespread, persistent, or rapidly progressive Erythema annulare that is unresponsive to topical treatments, systemic therapies may be considered. These are typically reserved for refractory cases due to their potential side effects. Systemic corticosteroids, such as oral prednisone, may be used for a short course to control acute flares or widespread inflammation, but long-term use is generally avoided. Other systemic agents that have been anecdotally reported or studied in small series include antimalarials (e.g., hydroxychloroquine), dapsone, phototherapy (UVB or PUVA), and immunosuppressants (e.g., methotrexate). These systemic treatments require careful consideration of the risk-benefit profile and continuous monitoring by a dermatologist. Supportive measures, such as avoiding known irritants, wearing loose-fitting clothing, and keeping the skin moisturized, can also help to manage the discomfort associated with the rash. Patient education regarding the benign nature of the condition and its potential for spontaneous resolution is also a vital component of Erythema annulare treatment. The primary goal is to improve the patient’s quality of life by reducing symptoms and mitigating the cosmetic impact of the lesions. Continued monitoring for resolution or progression, and reassessment of treatment strategies, are key aspects of long-term management.
- Topical Treatment Modalities:
- Topical Corticosteroids:
- Mechanism: Potent anti-inflammatory and immunosuppressive effects.
- Application: Applied directly to the active borders of the lesions, usually once or twice daily.
- Potency: Mild-to-moderate potency for initial treatment; higher potency for recalcitrant lesions under medical guidance.
- Examples: Hydrocortisone (mild), triamcinolone (moderate), clobetasol (high).
- Considerations: Risk of skin atrophy, striae, and telangiectasias with prolonged high-potency use.
- Topical Calcineurin Inhibitors (TCIs):
- Mechanism: Immunomodulatory agents that inhibit T-lymphocyte activation.
- Application: Alternative to corticosteroids, especially for sensitive areas.
- Examples: Tacrolimus ointment, pimecrolimus cream.
- Considerations: Less risk of corticosteroid-related side effects; may cause transient burning or itching.
- Topical Corticosteroids:
- Symptomatic Relief for Pruritus:
- Oral Antihistamines:
- Mechanism: Block histamine receptors, reducing itch sensation.
- Types: Non-sedating (e.g., loratadine, fexofenadine) for daytime; sedating (e.g., diphenhydramine, hydroxyzine) for nighttime.
- Use: Especially helpful if itching is a significant complaint.
- Emollients and Moisturizers:
- Mechanism: Hydrate the skin, improving barrier function and reducing dryness-related irritation.
- Use: General skin care to maintain skin health.
- Oral Antihistamines:
- Addressing Underlying Causes:
- Investigation: If a causal association (e.g., infection, drug reaction, malignancy) is suspected, diagnostic work-up is essential.
- Treatment of Primary Condition: Resolution of the underlying disorder may lead to the clearance of Erythema annulare.
- Drug Discontinuation: If drug-induced, cessation of the offending medication is paramount.
- Systemic Treatment Options (for severe/refractory cases):
- Systemic Corticosteroids:
- Use: Short courses for severe, widespread, or rapidly progressive disease.
- Considerations: Significant side effects with long-term use (e.g., weight gain, hypertension, diabetes, osteoporosis).
- Antimalarials:
- Example: Hydroxychloroquine.
- Use: Reported efficacy in some chronic cases, especially those resembling lupus.
- Considerations: Requires ophthalmologic screening due to risk of retinopathy.
- Dapsone:
- Mechanism: Anti-inflammatory and immunomodulatory properties.
- Use: Considered for recalcitrant cases.
- Considerations: Requires baseline G6PD enzyme testing and regular blood monitoring for hematological side effects.
- Phototherapy:
- Types: Narrowband UVB (nbUVB) or psoralen plus UVA (PUVA).
- Use: May be effective in some chronic, widespread forms.
- Considerations: Requires multiple sessions and carries risks of phototoxicity and skin cancer.
- Immunosuppressants:
- Example: Methotrexate, ciclosporin.
- Use: Rarely indicated for extremely severe, persistent cases unresponsive to other therapies, given their significant side effect profiles.
- Systemic Corticosteroids:
- Patient Education and Monitoring:
- Reassurance: Emphasize the benign and often self-limiting nature of the condition.
- Expectations: Manage expectations regarding treatment response and potential for recurrence.
- Follow-up: Regular dermatological review to monitor progression, assess treatment efficacy, and adjust therapy as needed.