Recognizing Diabetic foot symptoms pictures early is paramount for preventing severe complications and preserving limb health. This detailed guide aims to illustrate the diverse manifestations of diabetic foot, offering critical visual and descriptive insights for timely intervention and improved patient outcomes.
Diabetic foot Symptoms Pictures
The array of diabetic foot symptoms can be subtle at first, progressively worsening if left unaddressed. Understanding these indicators is crucial for proactive management and preventing severe complications like amputation. These symptoms are often a direct consequence of long-term elevated blood glucose levels, leading to nerve damage (neuropathy) and compromised blood circulation (peripheral artery disease or PAD).
Here are detailed descriptions of common diabetic foot symptoms:
- Numbness or Tingling (Neuropathy): One of the most common diabetic foot symptoms is a sensation of pins and needles, or complete numbness, particularly in the toes and feet. This diabetic neuropathy symptom arises from nerve damage, diminishing the ability to feel pain, temperature, or pressure. Patients might describe this as a “glove-and-stocking” distribution, where the sensation loss progresses upwards from the toes and feet, similar to wearing socks. The inability to feel minor cuts, blisters, or foreign objects in shoes significantly increases the risk of undetected injuries and subsequent infections.
- Burning Sensation: Paradoxically, while experiencing numbness, some individuals with diabetic neuropathy also report an intense burning pain in their feet, especially at night. This neuropathic pain symptom can range from a dull ache to sharp, excruciating pain, making sleep difficult and impacting daily life. The burning sensation is a sign of nerve irritation and malfunction, distinct from the typical musculoskeletal pain.
- Sharp Pains or Cramps: Intermittent sharp, shooting pains or muscle cramps in the feet and calves are frequently reported. These nerve pain symptoms can occur even at rest and are often exacerbated by activity. They reflect the erratic signaling of damaged nerves, leading to uncontrolled pain responses.
- Loss of Sensation (Protective Sensation Loss): A critical diabetic foot symptom is the gradual or complete loss of protective sensation. This means the foot can no longer adequately detect pressure, injury, or temperature extremes. A person might step on a sharp object, wear ill-fitting shoes that rub and cause blisters, or experience frostbite or burns without realizing it. This sensory deficit is a primary reason why minor foot injuries in diabetic patients often escalate rapidly into severe wounds.
- Weakness and Muscle Wasting: Motor neuropathy, affecting the nerves that control muscles, can lead to weakness and atrophy (wasting) of the small muscles in the feet. This muscle weakness symptom results in imbalances and deformities, such as claw toes or hammer toes, where the toes bend into an abnormal position. These deformities create new pressure points, increasing the risk of calluses and ulcers on the ball of the foot and the tips of the toes.
- Dry, Cracked Skin: Autonomic neuropathy affects the nerves controlling sweat glands and oil production in the skin. Consequently, the skin on the feet can become excessively dry, scaly, and prone to cracking, especially around the heels. These skin dryness symptoms are not just cosmetic; cracks in the skin provide easy entry points for bacteria, leading to infections. Reduced sweating also impairs the skin’s ability to regulate temperature and maintain its protective barrier.
- Formation of Thick Calluses: Due to altered foot biomechanics from muscle weakness and neuropathy, certain areas of the foot experience excessive pressure during walking. The body responds by building up layers of hard, thick skin known as calluses. While calluses are a protective response, in diabetic feet, they can become very thick, hard, and painful, often hiding deep ulcers underneath. These callus symptoms are common under the metatarsal heads (ball of the foot) and on the heels.
- Skin Discoloration: Changes in skin color are significant diabetic foot symptoms, often indicating circulatory problems or infection.
- Redness (Erythema): Localized redness can signal inflammation or infection, such as cellulitis, especially if accompanied by warmth and swelling.
- Bluish or Purplish Hue (Cyanosis): A bluish discoloration suggests poor oxygenation due to reduced blood flow, indicative of peripheral artery disease (PAD) or severe ischemia.
- Darkening of Skin (Hyperpigmentation): Chronic venous insufficiency can lead to brownish discoloration around the ankles, known as hemosiderin staining.
- Pale or Ashy Skin: Extremely pale or waxy-looking skin, particularly when the foot is elevated, can be a sign of severe arterial insufficiency.
- Swelling (Edema): Unilateral or bilateral swelling of the feet and ankles can be a diabetic foot symptom of several underlying issues. It might indicate infection (cellulitis), inflammation (Charcot foot), or circulatory problems (venous insufficiency or lymphedema). Persistent swelling can stretch the skin, making it more vulnerable to breakdown and ulceration, while also hindering healing.
- Open Sores or Ulcers: The most feared diabetic foot symptom is the development of non-healing ulcers. These diabetic ulcer symptoms typically occur on pressure points like the balls of the feet, the heels, or the tips of the toes. They often begin as minor cuts, blisters, or unnoticed calluses that break down. Diabetic ulcers are notoriously difficult to heal due to poor circulation, nerve damage, and susceptibility to infection. They can penetrate deep into tissues, involving tendons, bones, and joints, leading to osteomyelitis and eventually gangrene.
- Changes in Foot Shape (Charcot Arthropathy): A severe but often painless diabetic foot symptom is the progressive destruction of bones and joints in the foot, known as Charcot neuropathic osteoarthropathy (Charcot foot). This condition leads to rapid and severe deformity of the foot, often resulting in a “rocker-bottom” appearance. The foot may appear red, warm, and swollen, mimicking an infection, but it is primarily a neuro-osteoarthropathic process. Early detection of Charcot foot symptoms is vital to prevent irreversible damage.
- Pain or Cramping in Legs/Feet During Activity (Claudication): This peripheral artery disease symptom is characteristic of PAD. Individuals experience pain, cramping, or tiredness in their leg or foot muscles that develops during physical activity (e.g., walking) and subsides with rest. This is due to insufficient blood supply to the muscles during exertion. As PAD progresses, this pain can occur even at rest, particularly at night, and is a significant indicator of severe circulatory impairment.
Signs of Diabetic foot Pictures
Observing the physical signs of diabetic foot is paramount for early detection and intervention. Unlike subjective symptoms, signs are objective indicators visible during a physical examination or through diagnostic tests. These observable manifestations are critical for healthcare professionals and patients alike to monitor foot health effectively and identify potential problems before they escalate. Consistent self-examination and regular professional check-ups are key to recognizing these vital indicators.
Here are detailed descriptions of common diabetic foot signs:
- Redness and Warmth: Localized redness (erythema) and warmth to the touch are definitive signs of diabetic foot infection, particularly cellulitis. This indicates an inflammatory response, often to bacterial invasion. The redness might be diffuse or localized around a wound, and the area will feel distinctly warmer than the surrounding skin. In Charcot foot, the entire foot or ankle might appear intensely red and feel very warm, mimicking a severe infection.
- Swelling or Edema: Visible swelling of the foot or ankle is a significant observable diabetic foot sign. This edema can be unilateral (one foot) or bilateral (both feet). Causes range from acute infection (where swelling is typically localized and firm) to inflammation (as seen in Charcot foot, often diffuse and accompanied by warmth) to more chronic issues like venous insufficiency or fluid retention due to kidney problems. Persistent swelling compromises skin integrity and can mask underlying pathology.
- Visible Ulcers or Open Sores: The presence of an open sore or ulcer is a critical and easily identifiable diabetic foot sign. These typically appear on pressure points (e.g., sole of the foot under the metatarsal heads, heels, tips of toes, or areas prone to friction from footwear).
- Appearance: Diabetic ulcers can vary in size, depth, and appearance. They may present as a small crater, a deep cavity exposing bone or tendon, or a superficial wound.
- Exudate: Look for drainage (exudate) from the ulcer, which can be clear, bloody, purulent (pus, indicating infection), or malodorous. The color and consistency of the exudate provide clues about the type and severity of infection.
- Surrounding Skin: The skin around the ulcer may show signs of maceration (softening from moisture), callus formation (indicating chronic pressure), or discoloration (redness, pallor, or cyanosis).
- Granulation Tissue: Healthy ulcers will show pinkish-red granulation tissue at the base, indicating healing. Absence of this or the presence of slough (yellowish, stringy tissue) or eschar (black, necrotic tissue) suggests impaired healing or devitalized tissue.
- Nail Abnormalities: Toenails can display several diabetic foot signs.
- Thickened, Discolored Nails (Onychomycosis): Fungal infections are very common in diabetic feet, leading to nails that are thick, brittle, discolored (yellow, brown, or black), and crumbly.
- Ingrown Toenails: Poor nail trimming or tight footwear can cause ingrown toenails, which can easily become infected, especially in individuals with neuropathy who don’t feel the initial irritation.
- Ridges or Changes in Growth: Nutritional deficiencies or chronic illness can sometimes manifest as ridges or abnormal growth patterns in the nails.
- Loss of Hair on Toes and Feet: A significant sign of peripheral artery disease (PAD) is the absence of hair growth on the toes, dorsum (top) of the foot, or lower legs. This occurs due to poor circulation, as hair follicles do not receive adequate blood supply and nutrients to sustain growth. Shiny, atrophic skin often accompanies this sign.
- Shiny, Taut, or Thin Skin: Ischemic skin (skin with reduced blood supply) often appears shiny, thin, and stretched, particularly over the shins and feet. This skin texture sign results from the skin’s inability to receive proper nourishment and hydration due to compromised blood flow. It is more fragile and prone to breakdown.
- Diminished or Absent Pulses: Palpation of pedal pulses (dorsalis pedis and posterior tibial arteries) is a critical diagnostic sign of diabetic foot disease. Weak or absent pulses are strong indicators of peripheral artery disease (PAD), suggesting blockages in the arteries that supply blood to the feet. A Doppler ultrasound can be used to assess blood flow more accurately if pulses are difficult to palpate.
- Foot Deformities: Visual inspection can reveal various foot deformities that increase ulceration risk.
- Hammer Toes/Claw Toes: Toes that are abnormally bent or buckled, often due to muscle imbalance from neuropathy. These create pressure points on the tips or tops of the toes.
- Bunions: A bony bump that forms on the joint at the base of your big toe, often exacerbated by ill-fitting footwear.
- Charcot Foot Deformity: A severe and rapid collapse of the midfoot arch, leading to a “rocker-bottom” appearance. The foot may be widened, flattened, and severely misshapen, indicative of progressive joint destruction.
- Fissures or Cracks: Deep fissures or cracks, especially between the toes (due to moisture from sweat or poor drying) or on the heels (due to dry skin and pressure), are observable diabetic foot signs. These skin breaks create pathways for bacterial and fungal infections.
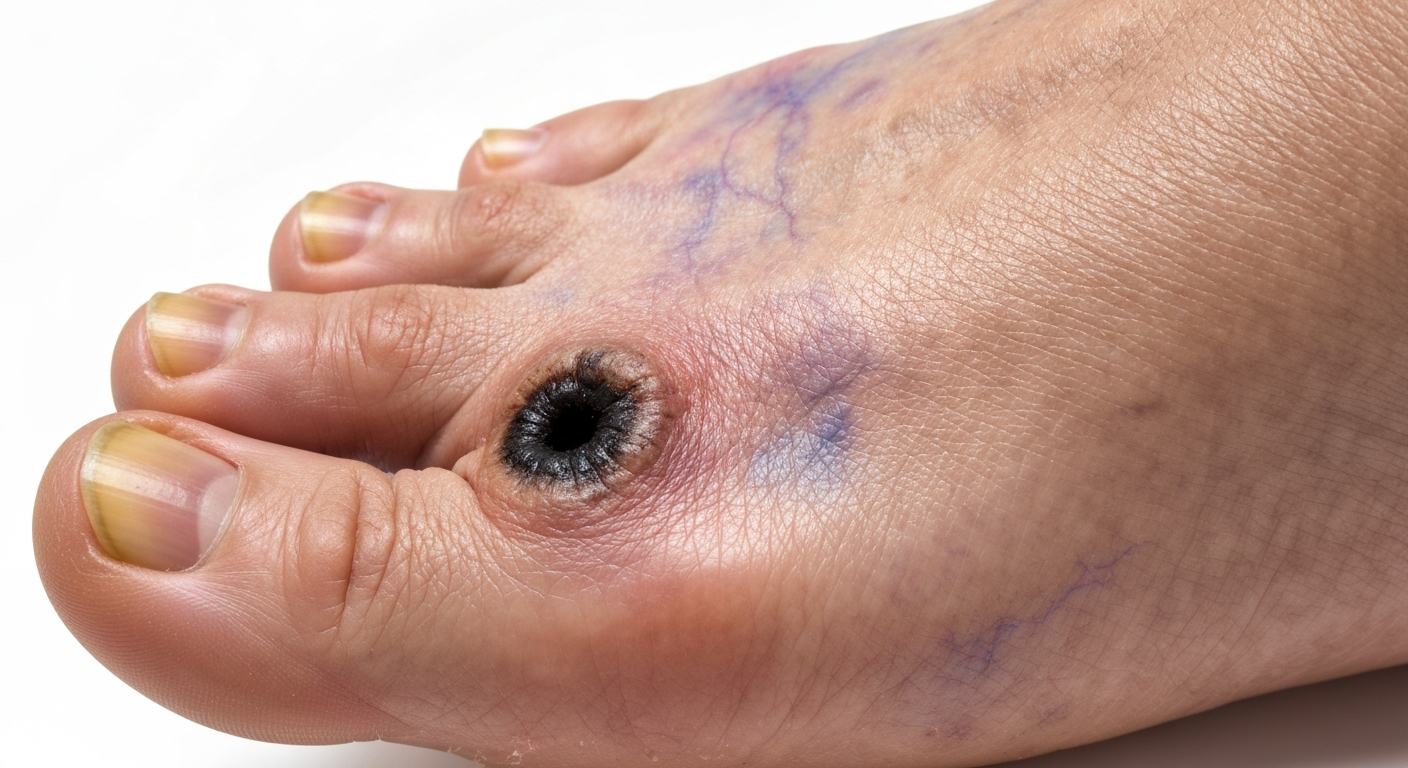
- Gangrene: The most severe and visually striking sign of diabetic foot disease is gangrene. This refers to the death of body tissue due to a lack of blood flow or a severe bacterial infection.
- Dry Gangrene: Appears as black, shriveled, mummified tissue, often starting at the toes. It’s typically a result of severe arterial insufficiency (lack of blood flow) and may not be painful if neuropathy is present.
- Wet Gangrene: Characterized by tissue that is swollen, blistering, and wet due to bacterial infection, often accompanied by a foul odor. It progresses rapidly and is a medical emergency.
Early Diabetic foot Photos
Identifying early Diabetic foot photos and their corresponding symptoms is pivotal for preventing the progression to severe complications. At this stage, changes can be subtle and easily overlooked, making vigilant self-care and professional screening essential. Early intervention can significantly alter the trajectory of diabetic foot disease, often preventing ulceration and infection. Paying close attention to minor alterations in foot appearance and sensation can make a profound difference in outcomes for individuals managing diabetes.
Here are detailed descriptions of early diabetic foot signs and symptoms:
- Minor Cuts, Scrapes, or Blisters That Don’t Heal Promptly: One of the earliest and most critical early diabetic foot signs is a small skin break that takes an unusually long time to heal, or worse, shows no signs of healing at all. This might be a tiny cut from a sharp object, a scrape from rubbing footwear, or a blister from new shoes. Due to impaired circulation and neuropathy, the normal inflammatory and healing responses are compromised. What would be a trivial injury for a healthy individual becomes a significant risk for a person with diabetes, as it can quickly become infected and deepen.
- Small, Unnoticeable Calluses or Corns: While calluses are often thought of as a sign of chronic pressure, the formation of new or slightly more prominent calluses or corns, especially in unusual areas or under the sole, can be an early diabetic foot symptom. These indicate subtle changes in foot mechanics or increased pressure points that, if not addressed, will inevitably lead to skin breakdown and ulceration beneath the hardened tissue.
- Dry, Flaky Skin on the Feet, Especially Heels: An early manifestation of autonomic neuropathy affecting sweat and oil glands is increasingly dry, flaky, or scaly skin on the feet. The skin may lose its natural suppleness and elasticity, leading to a dull or ashy appearance. This early skin symptom can precede visible cracks but indicates a compromised skin barrier, making the foot more susceptible to minor abrasions and pathogen entry.
- Subtle Changes in Skin Temperature: While severe infection causes obvious warmth, an early diabetic foot sign can be a slight, often localized, increase or decrease in skin temperature compared to the other foot or adjacent areas. A warm spot could indicate early inflammation or a developing infection, while a cooler area might suggest nascent circulatory impairment. These subtle variations are often only detectable by careful palpation.
- Intermittent Tingling or Burning Sensations: Initial nerve damage (neuropathy) often manifests as sporadic tingling, prickling, or a mild burning sensation in the toes or balls of the feet. These early neuropathy symptoms may come and go, perhaps more noticeable at night or after prolonged activity. They are a crucial warning that nerve function is starting to be compromised, even before significant loss of protective sensation occurs.
- Minor Changes in Toenail Appearance: Early fungal infections (onychomycosis) can cause slight discoloration (yellowish tint), thickening, or a crumbly texture at the edges of the toenails. An early nail symptom might also be an ingrown toenail that causes mild redness or discomfort, which, if ignored, can quickly lead to infection.
- A Feeling of “Walking on Cotton” or Reduced Sensitivity: Patients might describe a vague feeling of altered sensation, as if the ground beneath their feet isn’t quite as firm, or like their feet are “padded.” This early sensory loss symptom indicates the very beginning of sensory neuropathy, where the fine nerve endings are no longer transmitting signals effectively, leading to a diminished sense of touch or pressure, even if pain sensation is still largely intact.
- Small Areas of Redness or Irritation from Footwear: After wearing certain shoes, an early diabetic foot sign could be persistent small areas of redness or irritation that do not fade quickly. This indicates friction or pressure points that are not being adequately accommodated, often a precursor to blisters or skin breakdown. This is particularly important for individuals with early neuropathy who may not feel the discomfort of ill-fitting shoes.
- Slight Swelling After Prolonged Standing or Activity: While significant swelling is a later sign, an early diabetic foot symptom might be subtle, temporary swelling of the feet or ankles after extended periods of standing or walking. This could indicate early vascular issues or lymphatic dysfunction, and warrants attention as it increases the foot’s vulnerability.
- Slight Changes in Foot Temperature Regulation: Autonomic neuropathy can also affect the ability to regulate foot temperature. The feet may feel unusually cool or warm without an obvious cause, or one foot might feel consistently different from the other. This early thermal regulation symptom is often subtle and can precede more overt signs of autonomic dysfunction like excessive dryness.
Skin rash Diabetic foot Images
The skin on the feet of individuals with diabetes is highly susceptible to various dermatological conditions, often presenting as a skin rash diabetic foot. These rashes are frequently compounded by neuropathy, poor circulation, and a compromised immune system, making them more challenging to heal and more prone to severe complications. Recognizing these distinct skin manifestations is critical for targeted treatment and preventing progression to ulceration or systemic infection. Prompt identification and management of a skin rash diabetic foot is essential in comprehensive diabetic foot care.
Here are detailed descriptions of common skin rash diabetic foot conditions:
- Fungal Infections (Athlete’s Foot / Tinea Pedis):
- Appearance: This common diabetic foot rash presents as red, scaly, itchy patches, often accompanied by peeling skin, blisters, or fissures. It commonly affects the spaces between the toes, but can spread to the soles and sides of the feet. In diabetic patients, it can be more persistent and severe.
- Symptoms: Intense itching, burning, stinging, and sometimes a foul odor. The skin may appear macerated (soft and white) between the toes.
- Complications: Fissures created by Athlete’s foot provide easy entry points for bacteria, leading to secondary bacterial infections like cellulitis, particularly dangerous in neuropathic feet.
- Fungal Nail Infections (Onychomycosis):
- Appearance: While not a rash on the skin itself, diabetic nail fungus frequently accompanies other foot skin issues. Nails become thickened, discolored (yellow, brown, or black), brittle, and may crumble at the edges. The nail can lift from the nail bed.
- Symptoms: Often painless unless the nail becomes severely ingrown or causes pressure.
- Complications: Thickened nails can press against shoes, causing skin irritation and potentially leading to ulceration. They also harbor fungi that can spread to the surrounding skin.
- Bacterial Infections (Cellulitis):
- Appearance: A rapidly spreading diabetic foot rash characterized by diffuse redness, warmth, swelling, and tenderness of the skin and subcutaneous tissue. The borders of the affected area are typically indistinct, unlike some fungal rashes.
- Symptoms: Localized pain, fever, chills, malaise. The skin might appear shiny and stretched.
- Complications: Can quickly lead to deeper tissue infections, abscess formation, osteomyelitis, and sepsis if not treated promptly with appropriate antibiotics.
- Erysipelas:
- Appearance: A specific type of superficial cellulitis with a sharply defined, raised, red, warm, and tender border. It is often caused by Streptococcus bacteria.
- Symptoms: Similar to cellulitis but often with more distinct demarcation. High fever and chills can be prominent.
- Complications: Can spread rapidly, causing similar complications to cellulitis.
- Diabetic Dermopathy (“Shin Spots”):
- Appearance: Not strictly a rash, but a common diabetic skin condition. These appear as small, round or oval, brown, atrophic (sunken) spots, typically on the shins. They result from changes in small blood vessels and trauma to the skin.
- Symptoms: Usually asymptomatic, but can be mistaken for scars.
- Complications: Generally benign, but their presence indicates long-standing diabetes and microvascular complications.
- Necrobiosis Lipoidica Diabeticorum (NLD):
- Appearance: A rare but distinctive diabetic foot skin lesion. Starts as small, red-brown, raised papules that slowly expand into larger, shiny, thin, atrophic plaques with a yellowish-brown center and reddish-purple borders. Visible blood vessels may be seen through the thin skin. Most common on the shins, but can occur on the feet.
- Symptoms: Usually painless, but the affected skin is very fragile and prone to ulceration if traumatized.
- Complications: Chronic ulcers on NLD lesions are difficult to heal and susceptible to infection.
- Bullosis Diabeticorum (Diabetic Blisters):
- Appearance: These are spontaneous, painless blisters that can range from a few millimeters to several centimeters in size. They typically appear on the dorsum of the feet and toes, or hands. The blisters contain clear fluid and heal without scarring.
- Symptoms: Asymptomatic, although the presence of blisters can be alarming.
- Complications: While usually benign, these diabetic blister rash can rupture, leaving an open wound that is vulnerable to infection, especially in a neuropathic foot.
- Candidiasis (Yeast Infections):
- Appearance: A diabetic rash caused by Candida yeast. Often seen in warm, moist areas such as between the toes (especially if hygiene is poor) or under the breasts, and in skin folds. It presents as bright red patches, sometimes with small pustules or satellite lesions.
- Symptoms: Intense itching, burning, and sometimes a cheesy discharge.
- Complications: Can lead to secondary bacterial infections if the skin barrier is broken.
- Contact Dermatitis:
- Appearance: An itchy, red, sometimes blistering diabetic foot rash caused by an allergic reaction to topical medications, shoe materials, or other substances. The pattern often mirrors the shape of the offending agent.
- Symptoms: Intense itching, burning, and sometimes swelling.
- Complications: Persistent scratching can break the skin, leading to infection.
- Pruritus (Itching):
- Appearance: While not a rash itself, generalized or localized itching is a common diabetic skin symptom. Constant scratching can lead to excoriations (skin lesions caused by scratching) and secondary infections.
- Symptoms: Unrelenting itchiness, often worse at night or in dry conditions.
- Complications: Skin breakdown from scratching can predispose to infection and ulceration.
Diabetic foot Treatment
Effective Diabetic foot treatment is a multifaceted approach aimed at preventing complications, promoting healing, and preserving limb function. Given the complex interplay of neuropathy, peripheral artery disease, and impaired immune response, treatment strategies must be comprehensive and individualized. Early and aggressive intervention is crucial to avert the progression from minor issues to severe, life-threatening conditions like deep infections, osteomyelitis, and amputation. The focus of diabetic foot treatment is not only on addressing existing problems but also on education and preventive measures to maintain long-term foot health.
Here are detailed descriptions of key components of diabetic foot treatment:
- Comprehensive Wound Care and Debridement:
- Assessment: Thorough evaluation of the wound’s size, depth, location, presence of infection, and underlying causes (neuropathy, ischemia, pressure).
- Debridement: Surgical removal of dead (necrotic) or infected tissue from the wound bed. This is critical for promoting healing and reducing bacterial load. Debridement can be surgical, enzymatic, autolytic, or mechanical.
- Dressings: Application of appropriate wound dressings that maintain a moist wound environment, absorb exudate, protect from contamination, and promote granulation tissue formation. Types include hydrogels, alginates, foams, hydrocolloids, and antimicrobial dressings.
- Frequent Dressing Changes: Regular changes are essential to monitor progress, re-debride if necessary, and prevent secondary infections.
- Offloading and Pressure Redistribution:
- Total Contact Cast (TCC): A gold standard for treating plantar diabetic foot ulcers, evenly distributing pressure across the entire foot and lower leg, preventing weight-bearing on the ulcer.
- Removable Cast Walkers (RCWs) / Orthoses: Customized boots or braces designed to reduce pressure on specific areas of the foot. Compliance is critical.
- Therapeutic Footwear: Prescription shoes with extra depth, wider toe boxes, and custom inserts (orthotics) to accommodate deformities and distribute pressure evenly, preventing new ulcers and protecting healed ones.
- Crutches/Wheelchairs: For severe cases or non-ambulatory patients, to completely offload the affected foot.
- Infection Management:
- Antibiotics: Targeted systemic antibiotics based on wound culture and sensitivity testing are essential for treating bacterial infections (cellulitis, osteomyelitis, abscesses). Broad-spectrum antibiotics may be initiated empirically.
- Antifungals: Topical or oral antifungal medications for treating fungal infections (tinea pedis, onychomycosis).
- Surgical Drainage: Incision and drainage of abscesses or pus collections to remove infected material and reduce pressure.
- Osteomyelitis Treatment: Often requires prolonged courses of antibiotics (4-6 weeks) and sometimes surgical debridement of infected bone.
- Revascularization (Improving Blood Flow):
- Angioplasty and Stenting: Minimally invasive procedures to open blocked or narrowed arteries using balloons and/or stents, improving blood flow to the foot.
- Bypass Surgery: A surgical procedure to reroute blood flow around blocked arteries using a graft from another part of the body or a synthetic tube.
- Atherectomy: A procedure to remove plaque from within the arteries.
- Purpose: Crucial for healing ischemic ulcers, reducing rest pain, and preventing amputation in patients with significant peripheral artery disease (PAD).
- Glycemic Control:
- Blood Glucose Management: Strict control of blood glucose levels through diet, exercise, oral medications, or insulin is fundamental. Poor glycemic control impairs healing, weakens the immune system, and exacerbates neuropathy and vascular disease.
- HbA1c Monitoring: Regular monitoring of HbA1c to assess long-term blood glucose control.
- Patient Education and Prevention:
- Daily Foot Inspections: Teaching patients to inspect their feet daily for cuts, blisters, redness, swelling, or any changes.
- Proper Foot Hygiene: Washing feet daily with lukewarm water, drying thoroughly (especially between toes), moisturizing dry skin (avoiding between toes), and appropriate nail care.
- Appropriate Footwear: Emphasizing wearing protective, well-fitting shoes and socks at all times, even indoors.
- Avoiding Self-Treatment: Warning against “bathroom surgery” for corns, calluses, or ingrown nails.
- Smoking Cessation: Counseling to stop smoking, which severely impairs circulation.
- Specialized Care and Multidisciplinary Team:
- Podiatrist: Essential for routine foot care, callus debridement, nail care, and management of ulcers and deformities.
- Endocrinologist/Diabetologist: For optimizing diabetes management.
- Vascular Surgeon: For assessing and treating peripheral artery disease.
- Infectious Disease Specialist: For severe or complex infections.
- Physical Therapist: For gait training, exercises, and rehabilitation post-surgery.
- Orthotist/Prosthetist: For custom footwear, orthotics, and prosthetic devices if amputation is necessary.
- Pain Management:
- Neuropathic Pain Treatment: Medications like gabapentin, pregabalin, tricyclic antidepressants (amitriptyline), or SNRIs (duloxetine) to manage burning or shooting neuropathic pain.
- Wound Pain Management: Appropriate analgesics for pain associated with ulcers or infections.
- Advanced Therapies for Non-Healing Wounds:
- Growth Factors: Topical application of recombinant human platelet-derived growth factor (PDGF) to stimulate healing.
- Hyperbaric Oxygen Therapy (HBOT): Delivering high concentrations of oxygen in a pressurized chamber to promote wound healing, particularly in ischemic wounds or refractory infections.
- Bioengineered Skin Substitutes: Applying living cellular constructs to wounds that are struggling to heal.
- Negative Pressure Wound Therapy (NPWT) / VAC Therapy: Using a vacuum dressing to continuously remove exudate, reduce edema, and promote granulation tissue formation.
- Surgical Interventions for Deformities:
- Corrective Surgery: For severe foot deformities (e.g., Charcot foot, hammer toes) that are causing recurrent ulceration and cannot be managed by conservative means.
- Amputation: As a last resort, when infection is uncontrolled, gangrene is widespread, or limb salvage is not possible, to save the patient’s life or improve quality of life. The goal is always to perform the most conservative amputation possible.