This resource provides a detailed look at atopic dermatitis in adults symptoms pictures, offering visual descriptions to help understand the varied manifestations of this chronic skin condition. Understanding these visual cues is crucial for recognizing the presentation of adult atopic dermatitis, aiding in earlier identification and management strategies.
atopic dermatitis in adults Symptoms Pictures
Adults experiencing atopic dermatitis symptoms often present with a complex array of clinical manifestations that can vary significantly in intensity and appearance. Recognizing these key indicators is vital for accurate diagnosis and effective management. The primary symptom, and often the most distressing, is intense pruritus. This relentless itching can be debilitating, often worsening at night, severely disrupting sleep patterns and contributing significantly to the individual’s overall distress and fatigue. The visible consequence of this itching is often excoriations, which are linear scratch marks that can range from superficial abrasions to deeper skin breaks, sometimes accompanied by crusting. These excoriations are clearly visible in many atopic dermatitis in adults symptoms pictures, highlighting the severity of the itching.
Beyond the itching, the skin itself undergoes characteristic changes. Xerosis, or extreme dryness, is nearly universal in adults with atopic dermatitis. The skin appears dull, rough, and flaky, often feeling tight and uncomfortable. This impaired skin barrier function contributes to the vulnerability of the skin to irritants and allergens. Erythema, or redness, is another consistent feature, presenting as patches of varying shades of red, from a faint pink blush to a fiery, angry red, depending on the severity of inflammation and the individual’s skin tone. In individuals with darker skin tones, erythema may manifest as dusky grey, purplish, or brownish hues, which can be challenging to identify without careful observation, yet are critical to recognizing in atopic dermatitis in adults symptoms pictures.
Further visual symptoms that contribute to the typical appearance of adult eczema include:
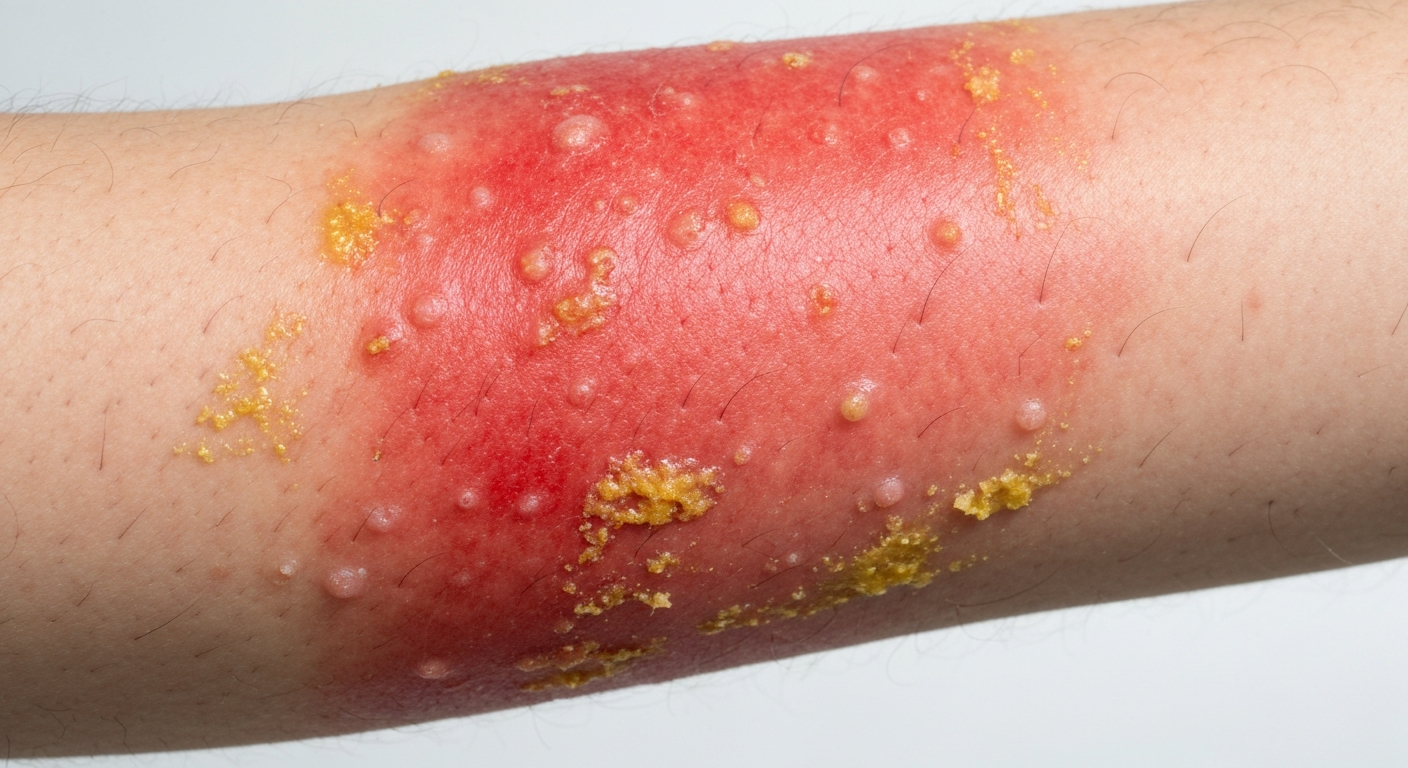
- Papules and Vesicles: Small, raised bumps (papules) and tiny, fluid-filled blisters (vesicles) are common during acute flares. These often break open, leading to weeping and crusting.
- Lichenification: A distinctive feature of chronic atopic dermatitis in adults. This is the thickening and hardening of the skin, with exaggerated skin markings, often described as having a leathery texture. It results from prolonged scratching and rubbing and is typically found in flexural areas like the elbows and knees.
- Edema (Swelling): During acute exacerbations, affected areas, particularly around the eyes, lips, or extremities, can become visibly swollen due to inflammation and fluid accumulation.
- Crusting and Oozing: These indicate more severe inflammation and often suggest secondary bacterial infection, characterized by yellowish or honey-colored crusts over open sores or weeping lesions.
- Scaling: The shedding of dry, flaky skin is pervasive, accompanying the underlying xerosis and inflammation.
- Hyperpigmentation: Post-inflammatory changes can lead to persistent darkening of the skin in affected areas, particularly noticeable in individuals with darker complexions. This post-inflammatory hyperpigmentation can linger long after the active rash has subsided, profoundly impacting cosmetic appearance.
- Hypopigmentation: Conversely, some areas, especially after prolonged inflammation, may become lighter than the surrounding skin, a condition known as post-inflammatory hypopigmentation or pityriasis alba. This is also more apparent in darker skin tones.
- Fissures: Cracks in the skin, especially in areas of chronic dryness, thickening, and movement (e.g., hands, feet, around joints), can be painful and prone to infection.
- Follicular Prominence: Hair follicles may become more prominent or inflamed, sometimes presenting as small, itchy bumps around the hair follicles (follicular eczema), more commonly observed in darker skin types.
These symptoms collectively paint a comprehensive picture of the challenges faced by adults with atopic dermatitis, and their visual representation in atopic dermatitis in adults symptoms pictures is invaluable for both patients and healthcare providers. The chronic nature of these symptoms significantly impacts quality of life, leading to psychological distress, social isolation, and occupational impairment.
Signs of atopic dermatitis in adults Pictures
When examining signs of atopic dermatitis in adults, clinicians look for specific physical findings that are indicative of the disease. These signs, often visible in signs of atopic dermatitis in adults pictures, go beyond the subjective symptoms and provide objective evidence of the skin’s inflammatory state and its response to chronic irritation. The distribution patterns of eczema in adults are highly characteristic. The flexural areas, such as the antecubital fossae (inner elbows), popliteal fossae (behind the knees), neck, wrists, and ankles, are classic sites for chronic atopic dermatitis. The skin in these areas often displays pronounced lichenification and erythema.
Other notable clinical signs include:
- Hand and Foot Eczema: This is a particularly common and often debilitating presentation in adults, characterized by redness, scaling, cracking, and intense itching on the palms, soles, and digits. It can sometimes manifest as dyshidrotic eczema (pompholyx), which involves deep-seated, intensely itchy vesicles (blisters) on the palms and soles, often preceding peeling.
- Periorbital and Perioral Involvement: Redness, scaling, and fissuring can affect the skin around the eyes (periorbital) and mouth (perioral). This includes the presence of “atopic shiners,” which are dark circles under the eyes caused by increased vascularity and inflammation, and Dennie-Morgan folds, which are extra skin folds under the lower eyelids. Cheilitis, characterized by dry, cracked, and inflamed lips, is also a common sign.
- Nipple Eczema: Persistent itching, redness, scaling, and sometimes cracking of the nipples, which can be misdiagnosed if atopic dermatitis is not considered.
- Follicular Atopic Dermatitis: As mentioned, this involves small, firm, itchy bumps concentrated around hair follicles, giving the skin a “goosebump” like appearance. It is more prevalent in individuals with skin of color.
- Pustules: The presence of pus-filled bumps often signals a secondary bacterial infection, or impetiginization, requiring specific antibiotic treatment.
- Dermatographism: A hypersensitive skin response where stroking or scratching the skin causes a raised, red wheal to appear. While not exclusive to atopic dermatitis, it’s a common finding. Some adults with AD may exhibit white dermatographism, where the scratched area turns pale due to vasoconstriction, a paradoxical response.
- Ichthyosis Vulgaris: An associated genetic condition characterized by widespread dry, scaly skin resembling fish scales, often more prominent on the lower legs. This condition exacerbates the xerosis seen in atopic dermatitis.
- Keratosis Pilaris: Another associated condition presenting as small, rough bumps, often on the upper arms, thighs, and buttocks. These bumps are due to keratin plugs in hair follicles.
- Hair Loss (Alopecia): In areas of severe and chronic inflammation or constant scratching, hair thinning or loss can occur, particularly on the scalp or eyebrows.
- Ocular Manifestations: Beyond periorbital eczema, adults with atopic dermatitis have a higher incidence of conjunctivitis, keratoconus (thinning of the cornea), and cataracts.
- Nail Changes: Nails may show signs of chronic scratching, such as polishing (shiny nails from rubbing) or dystrophy (ridging, pitting, or thickening). In some cases, chronic hand eczema can also impact nail health, leading to brittle or ridged nails.
These diverse signs, when observed in signs of atopic dermatitis in adults pictures, underscore the systemic impact of the disease and its potential to affect various body parts beyond the classic flexural folds. The detailed observation of these signs helps in assessing disease severity and guiding treatment strategies for adult eczema. The chronicity of these inflammatory processes means that many adults will present with a mixture of acute and chronic lesions, complicating the visual presentation but further confirming the diagnosis of chronic atopic dermatitis.
Early atopic dermatitis in adults Photos
Identifying early atopic dermatitis in adults through photos can be challenging, as the initial presentation might be subtle or mimic other skin conditions. However, understanding the nascent stages is crucial for prompt intervention to prevent progression and severe flares. Unlike in infants, where facial and scalp involvement is common, early atopic dermatitis in adults often begins in more localized areas or manifests as non-specific symptoms before a full-blown rash develops. Early atopic dermatitis in adults photos would typically capture the first visible inflammatory responses.
The initial signs often include:
- Acute Erythema and Pruritus: A sudden onset of localized redness accompanied by intense itching is frequently the first indication. This might appear as a transient red patch that is disproportionately itchy for its size. The skin might feel warm to the touch.
- Papular Eruptions: Small, red, itchy bumps (papules) can be among the earliest visible lesions. These might appear clustered in areas prone to sweating or friction, such as the inner elbows or behind the knees, even before significant lichenification sets in.
- Subtle Dryness and Sensitivity: Before the development of visible inflammation, adults might report increased dryness of certain skin areas or heightened sensitivity to common irritants like soaps, detergents, or fabrics. This precedes the visible signs of skin barrier dysfunction.
- Localized Patches of Inflammation: Rather than a generalized rash, early adult atopic dermatitis might start as a small, well-demarcated patch of redness and scaling in an area like the neck, wrist, or ankle. These patches might wax and wane initially.
- Mild Weeping or Vesiculation: In some acute early flares, particularly in highly sensitive individuals, small vesicles or blisters may quickly form, rupture, and ooze, leading to a wet appearance before crusting develops. This rapid progression from redness to weeping can be observed in early atopic dermatitis in adults photos if captured promptly.
- Unexplained, Persistent Itching: Sometimes, intense itching is experienced without a clear visible rash, leading to a “pre-eczematous” state. The scratching, however, eventually leads to visible excoriations and inflammation.
- Minimal Excoriations: Even in the early stages, the compelling urge to scratch can result in initial linear excoriations, which are fine scratch marks that can lead to further inflammation and infection if not managed.
- Color Variations in Early Lesions: In lighter skin tones, early lesions might be a bright pink or red. However, in individuals with darker skin tones, early inflammation might appear as subtle brownish, purplish, or greyish patches, which can make early identification more challenging. These color changes are critical to note in early atopic dermatitis in adults photos.
- “Fuzzy” or Ill-Defined Borders: Unlike some other dermatoses with sharp borders, early atopic dermatitis lesions can sometimes have poorly defined edges, gradually blending into the surrounding healthy skin.
The appearance of early atopic dermatitis in adults photos emphasizes the need for vigilance, especially in individuals with a personal or family history of atopy. Early recognition allows for the implementation of foundational skin barrier care and topical treatments, which can significantly reduce the severity and frequency of future flares, thereby altering the natural course of the disease and improving long-term outcomes for adult eczema patients.
Skin rash atopic dermatitis in adults Images
The skin rash of atopic dermatitis in adults is remarkably diverse, reflecting the chronic and fluctuating nature of the disease. Observing various forms of skin rash atopic dermatitis in adults images is essential for comprehending its multifaceted presentation. The appearance of the rash can range from acute, weeping lesions to chronic, thickened plaques, often coexisting on the same individual.
Key characteristics of the skin rash atopic dermatitis in adults include:
- Classic Eczematous Lesions: These are the most common presentations. In acute flares, the rash appears as erythematous (red) patches and plaques that are often edematous (swollen), with clusters of small papules and vesicles. These lesions frequently weep clear fluid and develop yellowish crusts, especially after scratching. The borders of the rash are typically ill-defined, blending into the surrounding skin.
- Lichenified Plaques: A hallmark of chronic adult atopic dermatitis, these are thick, leathery, and often hyperpigmented patches resulting from prolonged rubbing and scratching. The skin lines within these plaques are exaggerated, giving a corrugated appearance. These are commonly found in flexural areas (inner elbows, behind knees), the nape of the neck, wrists, and ankles, and are distinctively captured in skin rash atopic dermatitis in adults images.
- Nummular Eczema: This is a specific pattern of eczema, frequently seen in adults, characterized by coin-shaped (nummular) or oval lesions. These patches are typically erythematous, intensely itchy, scaly, and sometimes vesicular or crusted. They most often occur on the limbs, particularly the lower legs, and can be quite resistant to treatment. The distinct circular shape makes them identifiable in skin rash atopic dermatitis in adults images.
- Hand and Foot Eczema (Vesicular or Dry): The rash on the hands and feet can be particularly challenging. It may present as dry, scaly, fissured, and hyperkeratotic plaques (thickened skin) or as acute dyshidrotic eczema with deep-seated, intensely itchy blisters that later peel and crack. This can severely impair manual dexterity and mobility, impacting daily activities and employment.
- Follicular Eczema: More common in individuals with darker skin, this rash manifests as small, itchy papules concentrated around hair follicles, sometimes leading to pseudofolliculitis. It can be widespread across the trunk and extremities, presenting a bumpy, rough texture.
- Eczema Herpeticum (Kaposi’s Varicelliform Eruption): This is a severe, widespread secondary infection of eczematous skin with the Herpes Simplex Virus (HSV). The rash consists of monomorphic (uniform) punched-out erosions, vesicles, and pustules, often with central umbilication (a small indentation), that can spread rapidly. This is a medical emergency and its appearance in skin rash atopic dermatitis in adults images demands immediate clinical attention.
- Infected Eczema: Secondary bacterial infections, most commonly by Staphylococcus aureus, are frequent. The rash will show signs of infection such as increased redness and warmth, painful pustules, honey-colored crusting (impetiginization), and sometimes foul odor. This exacerbates the underlying atopic dermatitis and requires specific antimicrobial treatment.
- Generalized Erythroderma: In rare and severe cases, adult atopic dermatitis can progress to erythroderma, where more than 90% of the body surface is covered in redness, scaling, and shedding of skin. This is a life-threatening condition requiring hospitalization.
- Periorbital/Perioral Eczema: Delicate areas around the eyes and mouth often display fine scaling, erythema, and fissuring. The skin here is thinner and more susceptible to inflammation and dryness.
- Pityriasis Alba: Post-inflammatory hypopigmented patches, often with fine scaling, particularly on the face and arms. These are more visible in individuals with darker skin and represent areas where inflammation has temporarily disrupted melanin production.
The varied morphology and distribution of the skin rash atopic dermatitis in adults images underscore the importance of a thorough clinical evaluation. Each presentation provides clues about the chronicity, severity, and potential complications of the disease, guiding the choice of appropriate therapeutic interventions. The chronic inflammation and repeated cycles of healing and flaring leave lasting marks on the skin, contributing to the complex appearance of adult eczema.
atopic dermatitis in adults Treatment
Effective atopic dermatitis in adults treatment involves a multi-pronged approach aimed at controlling symptoms, restoring the skin barrier, preventing flares, and managing associated complications. Given the chronic nature of adult eczema, treatment plans are often long-term and individualized, requiring consistent adherence and close collaboration between the patient and healthcare provider. The goal is to improve the quality of life significantly, reducing the burden of symptoms often depicted in atopic dermatitis in adults symptoms pictures.
The primary pillars of atopic dermatitis in adults treatment include:
- Skin Barrier Restoration and Hydration:
- Emollients and Moisturizers: The cornerstone of daily management. These should be applied liberally and frequently (at least twice daily) to damp skin, ideally immediately after bathing. Ointments are generally preferred for very dry skin due to their occlusive properties, while creams are also effective. Key ingredients to look for include ceramides, hyaluronic acid, glycerin, shea butter, and other lipid-rich compounds that help replenish the skin’s natural barrier.
- Therapeutic Baths: Lukewarm (not hot) baths, kept short (5-10 minutes), followed immediately by “soak and seal” – gently patting dry and applying moisturizer while the skin is still damp. Additives like colloidal oatmeal can soothe itching, and diluted bleach baths (refer to clinical guidelines for concentration) can help reduce bacterial colonization on the skin, which is often a trigger for flares.
- Humidifiers: Maintaining optimal humidity indoors, especially during dry seasons or in arid climates, can help prevent skin from drying out further.
- Topical Anti-inflammatory Medications:
- Topical Corticosteroids (TCS): These remain the frontline treatment for acute flares. They come in various strengths (mild to super potent) and formulations. Potent TCS are used for short durations during flares in affected areas, while milder steroids may be used for sensitive skin areas (face, groin) or for maintenance. Education on proper application and potential side effects (e.g., skin thinning, telangiectasias) is crucial to prevent corticosteroid phobia.
- Topical Calcineurin Inhibitors (TCIs): Pimecrolimus cream and tacrolimus ointment are non-steroidal options effective for mild to moderate atopic dermatitis, particularly suitable for sensitive areas like the face, eyelids, and skin folds where TCS may cause side effects. They are also used for proactive maintenance therapy.
- Topical Phosphodiesterase 4 (PDE4) Inhibitors: Crisaborole ointment is a non-steroidal anti-inflammatory medication approved for mild to moderate atopic dermatitis. It provides another option for managing adult eczema, especially in areas where steroid use is limited.
- Topical Janus Kinase (JAK) Inhibitors: Ruxolitinib cream is a newer topical therapy that targets the JAK-STAT pathway involved in inflammation. It is used for short-term and non-continuous chronic treatment of mild to moderate atopic dermatitis.
- Systemic Therapies for Moderate-to-Severe Atopic Dermatitis:
- Oral Corticosteroids: Used sparingly for severe, widespread acute flares due to their rapid efficacy, but their long-term use is limited by significant systemic side effects. Short courses are typically tapered down.
- Traditional Immunosuppressants: Cyclosporine, methotrexate, azathioprine, and mycophenolate mofetil are used for adults with severe or refractory atopic dermatitis who do not respond to topical treatments or phototherapy. These require careful monitoring for side effects.
- Biologics: These are targeted antibody therapies that block specific inflammatory pathways. Dupilumab (IL-4/IL-13 inhibitor) and tralokinumab (IL-13 inhibitor) are approved for moderate-to-severe atopic dermatitis in adults who have not responded to other systemic treatments. They are administered via injection.
- Oral Janus Kinase (JAK) Inhibitors: Upadacitinib and abrocitinib are newer oral small molecule drugs that target the JAK-STAT pathway, offering significant relief for moderate-to-severe atopic dermatitis. These agents have demonstrated rapid efficacy but require careful patient selection and monitoring due to potential side effects.
- Antipruritics:
- Oral Antihistamines: Sedating antihistamines (e.g., hydroxyzine, diphenhydramine) can be helpful for nocturnal itching, aiding sleep. Non-sedating antihistamines are generally less effective for the specific itch of atopic dermatitis but may be used if concomitant urticaria is present.
- Gabapentin/Pregabalin: In some cases of severe, chronic, or neuropathic pruritus, these medications may be prescribed off-label.
- Anti-infective Treatments:
- Topical Antibiotics: For localized secondary bacterial infections.
- Oral Antibiotics: For widespread or severe secondary bacterial infections (e.g., impetiginized eczema) or suspected cellulitis.
- Antivirals: For suspected or confirmed eczema herpeticum (e.g., acyclovir, valacyclovir).
- Antifungals: If concomitant fungal infections are identified, especially in skin folds.
- Phototherapy:
- Narrowband UVB (NBUVB): Often used for moderate-to-severe atopic dermatitis when topical treatments are insufficient. It involves exposure to specific wavelengths of ultraviolet B light under medical supervision. UVA/UVB combination therapy is also an option.
- Lifestyle Modifications and Adjuvant Therapies:
- Trigger Avoidance: Identifying and avoiding known triggers such as specific allergens (dust mites, pet dander, pollen), irritants (harsh soaps, perfumes, wool), extreme temperatures, excessive sweating, and stress.
- Stress Management: Techniques like mindfulness, meditation, yoga, and psychotherapy can help manage stress, which is a known exacerbating factor for atopic dermatitis.
- Dietary Interventions: Generally, dietary restrictions are not recommended unless a specific food allergy is confirmed to trigger flares by an allergist.
- Clothing Choices: Wearing loose-fitting, soft, breathable fabrics like cotton can reduce irritation.
- Patient Education and Support: Comprehensive education on skin care routines, medication use, disease management, and access to support groups can significantly empower adults with atopic dermatitis to better manage their condition.
The comprehensive atopic dermatitis in adults treatment approach aims to reduce inflammation, alleviate itching, repair the skin barrier, and prevent complications, ultimately improving the lives of individuals living with this chronic skin condition. Regular follow-ups with a dermatologist are crucial to adjust treatment strategies as the disease evolves.